One of the most highly contagious diseases in humans is the measles. It is caused by a virus that invades the tissues of the respiratory system, particularly the lungs and throat passages. The most visible sign of measles is a rash that covers the face and body during the course of the disease. Although adults can get measles, it is more common in children. Measles is also known by the name rubeola.
How measles is spread
When a person infected with the measles virus coughs or sneezes, thousands of tiny particles of the virus are spread into the air. If an uninfected and unvaccinated person inhales these, he or she will become immediately infected. The virus particles make themselves at home in the moist passages of the nose, throat, and lungs.
Symptoms
The first symptoms, or signs, of measles appear about 10 to 14 days after a person is exposed to the measles virus. The earliest signs of the disease resemble those of the flu. The patient has a runny nose, a sore throat, and a fever. The fever is usually very high, sometimes as high as 104 ° or 105 ° F (40 ° C). The lining of the eyes becomes inflamed and very red. This condition is called conjunctivitis. Tiny bluish white spots appear on the insides of the cheeks. Within several days, a red rash appears on the face and behind the ears. The rash then spreads to the rest of the body.
For most patients, the symptoms of the disease do not go any further. In some patients, however, complications can occur. These include pneumonia, an illness that occurs when the lungs become infected. The measles virus can also attack the brain, causing an illness called encephalitis. This complication can cause the patient to have convulsions, or to go into a coma. If the virus infects the liver, it can cause the disease hepatitis. All of these complications are very serious. In some instances, they can be fatal.
Treatment
A case of the measles generally lasts 10 to 12 days, though with complications it will last much longer. The patient must get plenty of rest and drink fluids. Some people who are infected with the measles find bright light to be painful. In these cases, the patient's room should be kept dark. Because of the danger of complications, and also because measles is so easily spread, it is extremely important for the patient to stay home until completely recovered.
Prevention
When a disease is as contagious as measles, it is very important to prevent it from spreading and becoming an epidemic. An epidemic occurs when large numbers of people are infected with the same disease within a short period of time. Epidemics can spread across cities, states, and continents, and they can even spread around the world.
One way to prevent the spread of disease is through vaccination, or the use of substances that prevent people from getting the disease. Scientists have developed a very effective vaccine against measles. The vaccine also protects against mumps and rubella (sometimes called German measles). It is usually given to children twice before they can attend school. In the United States, the vaccine is widely available. In some countries, it is not available, and those countries suffer frequent epidemics. It is very important to discuss the vaccine, and the disease, with a doctor.
Tuesday, February 26, 2008
Epilepsy
Normally the brain's cells communicate with other cells by firing tiny electrical signals. Sometimes something goes wrong, and the cells signal many times faster than normal. That abnormal signaling causes an attack called a seizure. Seizures usually include sudden, abnormal movements and behaviors. People who have had two or more seizures have a condition called epilepsy.
Symptoms
The main symptom, or sign, of epilepsy is the seizure. There are two types of seizures: generalized and partial. Generalized seizures result from abnormal signals in most of the brain. Partial seizures result from abnormal signals in part of the brain.
During a generalized seizure the person may fall down and lose consciousness. The muscles may jerk, turn stiff, or become limp for a few minutes. Breathing can stop temporarily. After a violent seizure the person feels confused and tired. In some cases a generalized seizure is hard to notice. The person may just lose consciousness for a few seconds and stare or blink.
During a partial seizure the person does not usually fall down. The person may have sudden emotions or see, taste, or smell things that are not real. The person may seem to be in a dream. The muscles on one side of the body may jerk, or the person may repeat strange movements.
Causes
Many different things can cause epilepsy. It may result from a brain injury, either before or after birth, or a brain tumor. Diseases that affect the brain, including meningitis and encephalitis, can also lead to epilepsy. Epilepsy can sometimes occur after a person has a stroke (a blot clot or bleeding in the brain). Some cases of epilepsy may be genetic, or passed down from parent to child. In about half the cases of epilepsy the actual cause is not known.
Prevention
Because the cause of epilepsy is often unknown, the condition is difficult to prevent. People can prevent some types of epilepsy by protecting the brain from injury. Wearing a seat belt in cars can protect the head during an accident. Wearing a helmet while skating, biking, or playing sports can also prevent brain injury. Treating diseases and health problems that affect the brain can also help to prevent epilepsy.
Treatment
There is no cure for epilepsy, but there are a number of drugs that help to control seizures. A special diet can also help. If medicine and diet do not work, doctors may perform surgery on the brain. They may also place a small machine under the patient's skin. The machine sends electricity to the brain, which helps to reduce the number of seizures a person has.
People can help a person having a seizure by doing several things. They should help the person roll onto his side and put a pillow under his head. They should loosen the person's collar if possible. They should not put anything in the person's mouth. It is also important to move sharp or hard objects out of the person's way.
Symptoms
The main symptom, or sign, of epilepsy is the seizure. There are two types of seizures: generalized and partial. Generalized seizures result from abnormal signals in most of the brain. Partial seizures result from abnormal signals in part of the brain.
During a generalized seizure the person may fall down and lose consciousness. The muscles may jerk, turn stiff, or become limp for a few minutes. Breathing can stop temporarily. After a violent seizure the person feels confused and tired. In some cases a generalized seizure is hard to notice. The person may just lose consciousness for a few seconds and stare or blink.
During a partial seizure the person does not usually fall down. The person may have sudden emotions or see, taste, or smell things that are not real. The person may seem to be in a dream. The muscles on one side of the body may jerk, or the person may repeat strange movements.
Causes
Many different things can cause epilepsy. It may result from a brain injury, either before or after birth, or a brain tumor. Diseases that affect the brain, including meningitis and encephalitis, can also lead to epilepsy. Epilepsy can sometimes occur after a person has a stroke (a blot clot or bleeding in the brain). Some cases of epilepsy may be genetic, or passed down from parent to child. In about half the cases of epilepsy the actual cause is not known.
Prevention
Because the cause of epilepsy is often unknown, the condition is difficult to prevent. People can prevent some types of epilepsy by protecting the brain from injury. Wearing a seat belt in cars can protect the head during an accident. Wearing a helmet while skating, biking, or playing sports can also prevent brain injury. Treating diseases and health problems that affect the brain can also help to prevent epilepsy.
Treatment
There is no cure for epilepsy, but there are a number of drugs that help to control seizures. A special diet can also help. If medicine and diet do not work, doctors may perform surgery on the brain. They may also place a small machine under the patient's skin. The machine sends electricity to the brain, which helps to reduce the number of seizures a person has.
People can help a person having a seizure by doing several things. They should help the person roll onto his side and put a pillow under his head. They should loosen the person's collar if possible. They should not put anything in the person's mouth. It is also important to move sharp or hard objects out of the person's way.
Mumps
One of the most common and highly contagious diseases of childhood is mumps. This disease is caused by a virus that infects a pair of glands located in front of the ears. When the glands are infected, they become swollen. This gives the cheeks a chipmunk-like appearance. Although mumps can infect adults, it is more commonly found in children between the ages of 5 and 15 years
How mumps is spread
The glands that are infected by the mumps virus normally produce saliva. Because of this, when a person is infected, pieces of the virus become mixed in with the saliva produced by the glands. Any contact with the saliva of an infected person can therefore spread the disease.When an infected person coughs or sneezes, tiny particles of the virus are spread into the air. If these are inhaled by an uninfected person or a person who has not been vaccinated against the disease, that person will become ill with mumps. The disease can also be spread by touching something, such as bedding, that has infected saliva on it.
Symptoms
Once a person is infected with the mumps virus, it usually takes two to three weeks for symptoms, or signs of the disease, to appear. The first symptoms a patient will feel are very general and resemble those of the flu. The patient may have a runny nose and a slight fever. Soon the area in front of the ear becomes swollen and puffy. The swelling can spread to the upper neck and jaw. In most patients, the swelling is found on both sides of the face. The swelling is rarely severe, but sometimes the patient may have trouble chewing and swallowing.
Complications from mumps are rare but they can occur, particularly in older children. In some cases the meninges, a tissue that covers parts of the nervous system, can become inflamed. This leads to a disease called meningitis. Other complications can involve other glands in the body.
Treatment
The main symptoms of mumps—the swollen cheeks and neck—begin to go away after four or five days. There is no specific treatment for mumps. Because it is so contagious, patients should stay home. They should also get plenty of rest. Most patients can return to school or work after the swelling and other symptoms have gone away. However, it is always best to ask a doctor about this.
Prevention
Once a person is infected with mumps, he or she cannot get the disease again. This is called immunity. Another way to gain immunity from mumps is to be vaccinated against the disease. The vaccine used to protect against mumps is very effective. The same vaccine also protects against measles and rubella (also called German measles). Children in the United States usually receive this vaccine twice before they start school.
In some countries the vaccine is not as easily available. Those countries suffer frequent epidemics. This means that the disease spreads to large numbers of people within a short period of time. Epidemics can spread across cities, states, and continents, and they can even spread around the world. It is very important to prevent diseases like mumps from spreading and becoming an epidemic. One way to prevent this is by vaccination. It is very important to discuss the mumps vaccine, and the disease itself, with a doctor.
How mumps is spread
The glands that are infected by the mumps virus normally produce saliva. Because of this, when a person is infected, pieces of the virus become mixed in with the saliva produced by the glands. Any contact with the saliva of an infected person can therefore spread the disease.When an infected person coughs or sneezes, tiny particles of the virus are spread into the air. If these are inhaled by an uninfected person or a person who has not been vaccinated against the disease, that person will become ill with mumps. The disease can also be spread by touching something, such as bedding, that has infected saliva on it.
Symptoms
Once a person is infected with the mumps virus, it usually takes two to three weeks for symptoms, or signs of the disease, to appear. The first symptoms a patient will feel are very general and resemble those of the flu. The patient may have a runny nose and a slight fever. Soon the area in front of the ear becomes swollen and puffy. The swelling can spread to the upper neck and jaw. In most patients, the swelling is found on both sides of the face. The swelling is rarely severe, but sometimes the patient may have trouble chewing and swallowing.
Complications from mumps are rare but they can occur, particularly in older children. In some cases the meninges, a tissue that covers parts of the nervous system, can become inflamed. This leads to a disease called meningitis. Other complications can involve other glands in the body.
Treatment
The main symptoms of mumps—the swollen cheeks and neck—begin to go away after four or five days. There is no specific treatment for mumps. Because it is so contagious, patients should stay home. They should also get plenty of rest. Most patients can return to school or work after the swelling and other symptoms have gone away. However, it is always best to ask a doctor about this.
Prevention
Once a person is infected with mumps, he or she cannot get the disease again. This is called immunity. Another way to gain immunity from mumps is to be vaccinated against the disease. The vaccine used to protect against mumps is very effective. The same vaccine also protects against measles and rubella (also called German measles). Children in the United States usually receive this vaccine twice before they start school.
In some countries the vaccine is not as easily available. Those countries suffer frequent epidemics. This means that the disease spreads to large numbers of people within a short period of time. Epidemics can spread across cities, states, and continents, and they can even spread around the world. It is very important to prevent diseases like mumps from spreading and becoming an epidemic. One way to prevent this is by vaccination. It is very important to discuss the mumps vaccine, and the disease itself, with a doctor.
Influenza
The illness popularly known as the flu is one of the most common of the winter season. The word flu is short for the disease's full name, influenza. The disease is caused by a virus that invades the nose, throat, and lungs. In most cases, people who get the flu will recover in a week or so. In some instances, however, complications such as pneumonia can occur, leading to severe illness and even death.
How influenza is spread
In an infected person, the influenza virus lives in the tissue of the nose and lungs. When an infected person coughs or sneezes, tiny particles of the virus are released into the air, where they can be inhaled by another (uninfected) person. The virus quickly invades the tissues of the nose, migrating eventually to the throat and, finally, the lungs.
Influenza spreads quickly, especially in the winter, when many people are indoors. Because of this, an outbreak of influenza can quickly turn into an epidemic. Epidemics occur when large numbers of people are infected with the same disease within a short period of time. They can spread across cities, states, and continents, and they can even spread around the world. One of the worst epidemics of all time was the influenza epidemic of 1918–19. In one year, influenza killed more than 20 million people throughout the world. Other influenza epidemics have occurred since then, but none has been as deadly.
Symptoms
The initial symptoms, or signs of the disease, include body aches, chills, and fever. There may also be a sore throat and some coughing and sneezing. Patients often become extremely tired, and some may also experience sharp headache pain.
In some people—especially elderly people or very young children—infection with the influenza virus can lead to serious complications. These can include pneumonia and bronchitis, which are infections of the lungs or parts of the lungs. In some instances, infection with the influenza virus can lead to death.
Treatment
Treatment for influenza consists mainly of getting plenty of rest and drinking lots of fluids. Most people recover from a bout of influenza within one to two weeks. In the late 20th century, scientists developed medications that can treat influenza. However, in order for these medicines to work, they must be taken at the first sign of the disease. It is important to talk to a doctor about the illness and how it should be treated.
Children and teenagers should never use aspirin or aspirin-containing products to treat the headaches and body aches that accompany influenza. Using aspirin to treat influenza in children and teenagers has been connected to the development of a rare but serious illness called Reye syndrome.
Prevention
One of the best ways to avoid getting influenza is to be vaccinated against the influenza virus every year. Because the virus infects millions of people each year, getting vaccinated is also a good way to prevent the infection from spreading. For many diseases a single vaccine is all that is ever needed to protect against the virus. The influenza virus changes every year, however, so scientists must create new vaccines each year to protect against the new form of the virus.
How influenza is spread
In an infected person, the influenza virus lives in the tissue of the nose and lungs. When an infected person coughs or sneezes, tiny particles of the virus are released into the air, where they can be inhaled by another (uninfected) person. The virus quickly invades the tissues of the nose, migrating eventually to the throat and, finally, the lungs.
Influenza spreads quickly, especially in the winter, when many people are indoors. Because of this, an outbreak of influenza can quickly turn into an epidemic. Epidemics occur when large numbers of people are infected with the same disease within a short period of time. They can spread across cities, states, and continents, and they can even spread around the world. One of the worst epidemics of all time was the influenza epidemic of 1918–19. In one year, influenza killed more than 20 million people throughout the world. Other influenza epidemics have occurred since then, but none has been as deadly.
Symptoms
The initial symptoms, or signs of the disease, include body aches, chills, and fever. There may also be a sore throat and some coughing and sneezing. Patients often become extremely tired, and some may also experience sharp headache pain.
In some people—especially elderly people or very young children—infection with the influenza virus can lead to serious complications. These can include pneumonia and bronchitis, which are infections of the lungs or parts of the lungs. In some instances, infection with the influenza virus can lead to death.
Treatment
Treatment for influenza consists mainly of getting plenty of rest and drinking lots of fluids. Most people recover from a bout of influenza within one to two weeks. In the late 20th century, scientists developed medications that can treat influenza. However, in order for these medicines to work, they must be taken at the first sign of the disease. It is important to talk to a doctor about the illness and how it should be treated.
Children and teenagers should never use aspirin or aspirin-containing products to treat the headaches and body aches that accompany influenza. Using aspirin to treat influenza in children and teenagers has been connected to the development of a rare but serious illness called Reye syndrome.
Prevention
One of the best ways to avoid getting influenza is to be vaccinated against the influenza virus every year. Because the virus infects millions of people each year, getting vaccinated is also a good way to prevent the infection from spreading. For many diseases a single vaccine is all that is ever needed to protect against the virus. The influenza virus changes every year, however, so scientists must create new vaccines each year to protect against the new form of the virus.
Chicken pox
One of the most common diseases of childhood is chicken pox. This disease is caused by a virus. Although most patients contract it between the ages of 2 and 6, chicken pox can strike at any age. Chicken pox is a fairly mild illness in children. It can be very serious in adults, however. It is also extremely serious in people with certain diseases such as leukemia or AIDS because their immune systems are weak and therefore they cannot fight off the disease.
How chicken pox is spread
Chicken pox is highly contagious, meaning that it can spread very easily. When an infected person coughs or sneezes, tiny particles of the virus are released into the air. The disease can be spread when an uninfected person inhales these particles. The virus particles can also be on the clothing or bedding of an infected patient. If an uninfected person touches the clothing or bedding he or she can become infected with the disease.
Symptoms
The first symptoms, or signs of the disease, are very general and resemble those of the flu. These include a slight fever, runny nose, and mild cough. The patient will not feel very hungry and may also have headaches and feel very tired.
Roughly two weeks after being exposed to the virus, red spots appear on the face and body. These spots are filled with fluid, and they itch terribly. Eventually the spots form scabs, which soon fall off.
Treatment
People with chicken pox should try not to scratch the spots. Scratching can cause the spots to leave deep scars. The itching can be relieved by using medications such as calamine lotion, which has a soothing effect. In addition to using calamine lotion, patients may wish to bathe the pox spots and sores with cool water. It is important to keep the spots clean so that they do not become further infected with other harmful germs. Bed rest is important.
It is extremely important to never use aspirin or aspirin-containing products to treat the headaches and body aches that accompany chicken pox. Using aspirin to treat chicken pox has been connected to the development of a severe disease called Reye syndrome. This syndrome can cause liver and brain damage, and even death.
A case of chicken pox generally lasts from a week to ten days overall. Because the disease is so contagious, it is important for the patient to remain confined to bed until the scabs have fallen off. Complications are rare but can occur in some cases. In some instances, the virus becomes dormant. This means that it remains in the body but no longer causes the symptoms of chicken pox. In these cases, it is possible for the virus to become re-activated in adulthood, when it causes a related disease called shingles. Scientists developed a chicken pox vaccine, or substance that protects people from getting the disease, in the late 20th century.
How chicken pox is spread
Chicken pox is highly contagious, meaning that it can spread very easily. When an infected person coughs or sneezes, tiny particles of the virus are released into the air. The disease can be spread when an uninfected person inhales these particles. The virus particles can also be on the clothing or bedding of an infected patient. If an uninfected person touches the clothing or bedding he or she can become infected with the disease.
Symptoms
The first symptoms, or signs of the disease, are very general and resemble those of the flu. These include a slight fever, runny nose, and mild cough. The patient will not feel very hungry and may also have headaches and feel very tired.
Roughly two weeks after being exposed to the virus, red spots appear on the face and body. These spots are filled with fluid, and they itch terribly. Eventually the spots form scabs, which soon fall off.
Treatment
People with chicken pox should try not to scratch the spots. Scratching can cause the spots to leave deep scars. The itching can be relieved by using medications such as calamine lotion, which has a soothing effect. In addition to using calamine lotion, patients may wish to bathe the pox spots and sores with cool water. It is important to keep the spots clean so that they do not become further infected with other harmful germs. Bed rest is important.
It is extremely important to never use aspirin or aspirin-containing products to treat the headaches and body aches that accompany chicken pox. Using aspirin to treat chicken pox has been connected to the development of a severe disease called Reye syndrome. This syndrome can cause liver and brain damage, and even death.
A case of chicken pox generally lasts from a week to ten days overall. Because the disease is so contagious, it is important for the patient to remain confined to bed until the scabs have fallen off. Complications are rare but can occur in some cases. In some instances, the virus becomes dormant. This means that it remains in the body but no longer causes the symptoms of chicken pox. In these cases, it is possible for the virus to become re-activated in adulthood, when it causes a related disease called shingles. Scientists developed a chicken pox vaccine, or substance that protects people from getting the disease, in the late 20th century.
Rabies
also called hydrophobia , or lyssa acute, usually fatal, viral infectious disease of the central nervous system. The disease is usually spread among domestic dogs and wild carnivorous animals; all warm-blooded animals are susceptible to rabies infection. The virus, a rhabdovirus, is often present in the salivary glands of rabid animals and is excreted in the saliva; thus, the bite of the infected animal introduces the virus into a fresh wound. Under favourable conditions, the virus propagates along nerve tissue from the wound to the brain and becomes established in the central nervous system. The disease develops most often between four and six weeks after infection, but the incubation period may vary from 10 days to eight months.
Rabies often begins with excitation of the central nervous system expressed as irritability and viciousness. A rabid animal is most dangerous during the early stages of the disease because it appears to be healthy and may seem friendly but will bite at the slightest provocation. Wild animals that appear to be tame and that approach people or human habitations in the daytime should be suspected of having rabies.
Infected dogs usually show a short excitation phase that is characterized by restlessness, nervousness, irritability, and viciousness and is followed by depression and paralysis. Sudden death without recognizable signs of illness is common. Dogs that develop the predominantly excited type of rabies invariably die of the infection, usually within three to five days after the onset of symptoms. Those that develop the paralytic type of rabies without any evidence of excitation or viciousness may recover on rare occasions. Paralysis of the “voice” muscles in rabid dogs may produce a characteristic change in the sound of the bark.
Rabies in humans is similar to that in animals. Symptoms include depression, headache, nausea, seizures, anorexia, muscle stiffness, and increased production of saliva. Abnormal sensations, such as itching, around the site of exposure are a common early symptom. Repeated episodes of painful contraction of the muscles of the throat may occur upon attempting to swallow or may be elicited by the sight of water. This reaction to water is called hydrophobia (“fear of water”). Rabies in humans is almost always fatal. Death ordinarily occurs within three to five days after the onset of symptoms due to cardiac or respiratory failure. Sometimes rabies is characterized by paralysis without any evidence of excitation of the nervous system. In such cases the course of the disease may be prolonged to a week or more.
If administered soon after infection, serum or vaccine can be effective in combating the disease. This is a type of passive immunization whereby animals are immunized with attenuated rabies virus, and antibodies from these animals are injected into infected persons to give them temporary immunity to rabies. The treatment is effective if given within 24 hours after exposure but has little, if any, value if given three or more days after infection by rabies. Immediate treatment of animal-bite wounds by cleansing with soap and water is extremely important because much, if not all, of the virus can be thus removed.
Vaccines prepared from rabies virus can be used to protect people who are likely to be in contact with infected animals. The safest and most effective vaccines are human diploidcell vaccine (HDCV), purified chick embryo cell culture (PCEC), and rabies vaccine adsorbed (RVA). When a person not protected by previous immunization is bitten by a rabid animal, treatment is a dose of serum followed by a series of vaccinations. With the older vaccines, at least 16 injections were required, whereas with HDCV, PCEC, or RVA, 5 are usually sufficient.
Rabies often begins with excitation of the central nervous system expressed as irritability and viciousness. A rabid animal is most dangerous during the early stages of the disease because it appears to be healthy and may seem friendly but will bite at the slightest provocation. Wild animals that appear to be tame and that approach people or human habitations in the daytime should be suspected of having rabies.
Infected dogs usually show a short excitation phase that is characterized by restlessness, nervousness, irritability, and viciousness and is followed by depression and paralysis. Sudden death without recognizable signs of illness is common. Dogs that develop the predominantly excited type of rabies invariably die of the infection, usually within three to five days after the onset of symptoms. Those that develop the paralytic type of rabies without any evidence of excitation or viciousness may recover on rare occasions. Paralysis of the “voice” muscles in rabid dogs may produce a characteristic change in the sound of the bark.
Rabies in humans is similar to that in animals. Symptoms include depression, headache, nausea, seizures, anorexia, muscle stiffness, and increased production of saliva. Abnormal sensations, such as itching, around the site of exposure are a common early symptom. Repeated episodes of painful contraction of the muscles of the throat may occur upon attempting to swallow or may be elicited by the sight of water. This reaction to water is called hydrophobia (“fear of water”). Rabies in humans is almost always fatal. Death ordinarily occurs within three to five days after the onset of symptoms due to cardiac or respiratory failure. Sometimes rabies is characterized by paralysis without any evidence of excitation of the nervous system. In such cases the course of the disease may be prolonged to a week or more.
If administered soon after infection, serum or vaccine can be effective in combating the disease. This is a type of passive immunization whereby animals are immunized with attenuated rabies virus, and antibodies from these animals are injected into infected persons to give them temporary immunity to rabies. The treatment is effective if given within 24 hours after exposure but has little, if any, value if given three or more days after infection by rabies. Immediate treatment of animal-bite wounds by cleansing with soap and water is extremely important because much, if not all, of the virus can be thus removed.
Vaccines prepared from rabies virus can be used to protect people who are likely to be in contact with infected animals. The safest and most effective vaccines are human diploidcell vaccine (HDCV), purified chick embryo cell culture (PCEC), and rabies vaccine adsorbed (RVA). When a person not protected by previous immunization is bitten by a rabid animal, treatment is a dose of serum followed by a series of vaccinations. With the older vaccines, at least 16 injections were required, whereas with HDCV, PCEC, or RVA, 5 are usually sufficient.
Pompe's disease
also called Glycogenosis Type Ii, hereditary defect in the body's ability to metabolize glycogen, resulting in a muscle disorder that is usually fatal during the first year of life. The defect responsible, absence of the enzyme alpha-1,4-glucosidase, is extremely rare, occurring in fewer than one in every 150,000 births, and is transmitted as an autosomal recessive trait. In Pompe's disease, glycogen accumulates in all body tissues, but especially in the muscles, causing enlargement of the heart, cardiac muscle failure, and breathing difficulties. Accumulation of glycogen in other tissues causes mental retardation and enlargement of the liver and spleen. Death usually results from cardiorespiratory failure. Juvenile and adult forms, with similar but milder symptoms, are also known.
Simmonds' disease
pituitary disorder characterized by panhypopituitarism, a form of hypopituitarism in which all pituitary secretions are deficient. Effects include dwarfism, atrophy of the sex glands, shrinkage of the breasts and suppression of milk secretion, atrophy of the thyroid and the adrenal cortex, lowering of the metabolic rate, tendency toward lowered blood sugar, and lessened resistance to infection and shock. Some effects of panhypopituitarism have been simulated among emotionally deprived young children. Such children have shown remarkable recovery when removed from the injurious environment. The German doctor Morris Simmonds (1855–1925) first described this disease in 1914.
McArdle's disease
also called Glycogenosis Type V, rare hereditary deficiency of the enzyme glycogen phosphorylase in muscle cells. In the absence of this enzyme, muscles cannot break down animal starch (glycogen) to meet the energy requirements of exercise. Muscle activity is thus solely dependent on the availability of glucose (blood sugar) and other nutrients in the circulating blood. Victims of McArdle's disease are chronically weak because their muscles are incapable of prolonged exertion; even moderate exercise produces muscle cramping and severe pain. Unlike most other types of glycogenosis, the disease is not fatal, and the missing enzyme does not impair the functioning of other body systems. McArdle's disease is inherited as an autosomal recessive trait
Plummer's disease
also called toxic multinodular goitre thyroid condition characterized by marked enlargement of the thyroid gland (goitre), firm thyroid nodules, and mild overproduction of thyroid hormone (hyperthyroidism). Plummer's disease, which usually occurs in older people, is of unknown etiology. Its symptoms resemble those of Graves' disease (q.v.), a condition believed to be an autoimmune disorder caused by antibodies to the thyroid.
Typically, persons affected by Plummer's disease develop a goitre many years before the onset of symptoms of hyperthyroidism; most patients are over age 50 before the characteristic accelerated heart rate and other cardiac conditions appear. Unlike other forms of hyperthyroidism, the disease seldom causes bulging of the eyes (exophthalmos). Swelling of the thyroid gland may obstruct breathing or swallowing, requiring surgery to remove the excess tissue; the cardiac symptoms, resulting in congestive heart failure in some cases, can also be fatal. In the absence of obstruction or cosmetic reasons for removing the gland, the goitre may be treated with drugs that block thyroid activity or with radioactive iodine therapy; however, the multiple thyroid nodules characteristic of the disease may raise suspicion of cancer, necessitating surgical excision of the gland.
Typically, persons affected by Plummer's disease develop a goitre many years before the onset of symptoms of hyperthyroidism; most patients are over age 50 before the characteristic accelerated heart rate and other cardiac conditions appear. Unlike other forms of hyperthyroidism, the disease seldom causes bulging of the eyes (exophthalmos). Swelling of the thyroid gland may obstruct breathing or swallowing, requiring surgery to remove the excess tissue; the cardiac symptoms, resulting in congestive heart failure in some cases, can also be fatal. In the absence of obstruction or cosmetic reasons for removing the gland, the goitre may be treated with drugs that block thyroid activity or with radioactive iodine therapy; however, the multiple thyroid nodules characteristic of the disease may raise suspicion of cancer, necessitating surgical excision of the gland.
Huntington disease
also called Huntington chorea a relatively rare, and invariably fatal, hereditary neurological disease that is characterized by irregular and involuntary movements of the muscles. Huntington disease is caused by a genetic mutation that causes degeneration of neurons in the basal ganglia, a pair of nerve clusters deep within the brain, that control movement. Symptoms usually appear between the ages of 35 and 50 and worsen over time. They begin with occasional jerking or writhing movements, called choreiform movements, or what appear to be minor problems with coordination; these movements, which are absent during sleep, worsen over the next few years and progress to random, uncontrollable, and often violent twitchings and jerks. Symptoms of mental deterioration may appear including apathy, fatigue, irritability, restlessness, or moodiness; these symptoms may progress to memory loss, dementia, bipolar disorder, or schizophrenia. The disease was first described by the American physician George Huntington in 1872.
A child of someone with Huntington disease has a 50 percent chance of developing the disease; a genetic test is available. No effective therapy or cure is available for the disorder, although choreiform movements may be partially and temporarily suppressed by phenothiazines or other antipsychotic medications.
A child of someone with Huntington disease has a 50 percent chance of developing the disease; a genetic test is available. No effective therapy or cure is available for the disorder, although choreiform movements may be partially and temporarily suppressed by phenothiazines or other antipsychotic medications.
Alzheimer disease
degenerative brain disorder that develops in mid to late adulthood. It results in a progressive and irreversible decline in memory and a deterioration of various other cognitive abilities. The disease is characterized by the destruction of nerve cells and neural connections in the cerebral cortex of the brain and by a significant loss of brain mass. The disease was first described in 1906 by Alois Alzheimer, a German neuropathologist.
Alzheimer disease is the most common form of *dementia. The disease develops differently among individuals; this suggests that more than one pathologic process may lead to the same outcome. Typically, the first symptom to appear is forgetfulness. As the disease progresses, memory loss becomes more severe, and language, perceptual, and motor skills deteriorate. Mood becomes unstable, and the individual tends to become irritable and more sensitive to stress and may become intermittently angry, anxious, or depressed. In advanced stages, the individual becomes unresponsive and loses mobility and control of body functions; death ensues after a disease course lasting from 2 to 20 years.
About 10 percent of those who develop the disease are younger than 60 years of age. These cases, referred to as early-onset familial Alzheimer disease, result from an inherited genetic mutation. The majority of cases of Alzheimer disease, however, develop after age 60 (late-onset); they usually occur sporadically—i.e., in individuals with no family history of the disease—although a genetic factor has been identified that is thought to predispose these individuals to the disorder.
The presence of neuritic plaques and neurofibrillary tangles in the brain are used to diagnose Alzheimer disease in autopsy. Neuritic plaques—also called senile, dendritic, or amyloid plaques—consist of deteriorating neuronal material surrounding deposits of a sticky protein called beta amyloid. This protein is derived from a larger molecule called amyloid precursor protein, which is a normal component of nerve cells. Neurofibrillary tangles are twisted protein fibres located within nerve cells. These fibres consist of a protein, called tau, that normally occurs in neurons. When incorrectly processed, tau molecules clump together and form tangles. Both neuritic plaques and neurofibrillary tangles, which also may be found in smaller amounts in the brains of healthy elderly persons, are thought to interfere in some way with normal cellular functioning. However, it is not known whether the plaques and tangles are a cause or a consequence of the disease.
Other features have been noted in the brains of many persons with Alzheimer disease. One is a deficiency of the neurotransmitter acetylcholine; neurons containing acetylcholine play an important role in memory. Abnormal concentrations of aluminum also have been found in neurofibrillary tangles and neuritic plaques, but it is not known whether the element plays a causative role in the disease.
Underlying genetic defects have been identified for both late- and early-onset cases of Alzheimer disease. A defect in the gene that codes for amyloid precursor protein may increase the production or deposition of beta amyloid, which forms the core of neuritic plaques. This gene, however, is responsible for only 2 to 3 percent of all early-onset cases of the disease; the remainder are attributed to two other genes. A defect in the gene that directs production of apolipoprotein E (ApoE), which is involved in cholesterol transport, may be a factor in the majority of late-onset Alzheimer cases. There are three forms of this gene—ApoE2, ApoE3, and ApoE4—one of which, ApoE4, is associated with a higher risk of disease.
There is no cure for Alzheimer disease. The medication tacrine slightly slows the progression of the disease by slowing the breakdown of acetylcholine, but it is not effective in all patients and can become toxic to the liver. Most treatment aims to control the depression, behavioral problems, and insomnia that often accompany the disease.
*dementia
chronic, usually progressive deterioration of intellectual capacity associated with the widespread loss of nerve cells and the shrinkage of brain tissue. Dementia is most commonly seen in the elderly (senile dementia), though it is not part of the normal aging process and can affect persons of any age.
The most common irreversible dementia is Alzheimer disease. This condition begins with memory loss, which may first appear to be simple absentmindedness or forgetfulness. As dementia progresses, the loss of memory broadens in scope until the individual can no longer remember basic social and survival skills or function independently. Language, spatial or temporal orientation, judgment, or other cognitive capacities may decline, and personality changes may also occur. Dementia is also present in other degenerative brain diseases including Pick disease and Parkinson disease.
The second most common cause of dementia is hypertension (high blood pressure) or other vascular conditions. This type of dementia, called multi-infarct, or vascular, dementia results from a series of small strokes that progressively destroy the brain. Dementia can also be caused by Huntington disease, syphilis, multiple sclerosis, acquired immune deficiency syndrome (AIDS), and some types of encephalitis. Treatable dementias occur in hypothyroidism, other metabolic diseases, and some malignant tumours. Treatment of the underlying disease in these cases may inhibit the progress of dementia but usually does not reverse it.
Alzheimer disease is the most common form of *dementia. The disease develops differently among individuals; this suggests that more than one pathologic process may lead to the same outcome. Typically, the first symptom to appear is forgetfulness. As the disease progresses, memory loss becomes more severe, and language, perceptual, and motor skills deteriorate. Mood becomes unstable, and the individual tends to become irritable and more sensitive to stress and may become intermittently angry, anxious, or depressed. In advanced stages, the individual becomes unresponsive and loses mobility and control of body functions; death ensues after a disease course lasting from 2 to 20 years.
About 10 percent of those who develop the disease are younger than 60 years of age. These cases, referred to as early-onset familial Alzheimer disease, result from an inherited genetic mutation. The majority of cases of Alzheimer disease, however, develop after age 60 (late-onset); they usually occur sporadically—i.e., in individuals with no family history of the disease—although a genetic factor has been identified that is thought to predispose these individuals to the disorder.
The presence of neuritic plaques and neurofibrillary tangles in the brain are used to diagnose Alzheimer disease in autopsy. Neuritic plaques—also called senile, dendritic, or amyloid plaques—consist of deteriorating neuronal material surrounding deposits of a sticky protein called beta amyloid. This protein is derived from a larger molecule called amyloid precursor protein, which is a normal component of nerve cells. Neurofibrillary tangles are twisted protein fibres located within nerve cells. These fibres consist of a protein, called tau, that normally occurs in neurons. When incorrectly processed, tau molecules clump together and form tangles. Both neuritic plaques and neurofibrillary tangles, which also may be found in smaller amounts in the brains of healthy elderly persons, are thought to interfere in some way with normal cellular functioning. However, it is not known whether the plaques and tangles are a cause or a consequence of the disease.
Other features have been noted in the brains of many persons with Alzheimer disease. One is a deficiency of the neurotransmitter acetylcholine; neurons containing acetylcholine play an important role in memory. Abnormal concentrations of aluminum also have been found in neurofibrillary tangles and neuritic plaques, but it is not known whether the element plays a causative role in the disease.
Underlying genetic defects have been identified for both late- and early-onset cases of Alzheimer disease. A defect in the gene that codes for amyloid precursor protein may increase the production or deposition of beta amyloid, which forms the core of neuritic plaques. This gene, however, is responsible for only 2 to 3 percent of all early-onset cases of the disease; the remainder are attributed to two other genes. A defect in the gene that directs production of apolipoprotein E (ApoE), which is involved in cholesterol transport, may be a factor in the majority of late-onset Alzheimer cases. There are three forms of this gene—ApoE2, ApoE3, and ApoE4—one of which, ApoE4, is associated with a higher risk of disease.
There is no cure for Alzheimer disease. The medication tacrine slightly slows the progression of the disease by slowing the breakdown of acetylcholine, but it is not effective in all patients and can become toxic to the liver. Most treatment aims to control the depression, behavioral problems, and insomnia that often accompany the disease.
*dementia
chronic, usually progressive deterioration of intellectual capacity associated with the widespread loss of nerve cells and the shrinkage of brain tissue. Dementia is most commonly seen in the elderly (senile dementia), though it is not part of the normal aging process and can affect persons of any age.
The most common irreversible dementia is Alzheimer disease. This condition begins with memory loss, which may first appear to be simple absentmindedness or forgetfulness. As dementia progresses, the loss of memory broadens in scope until the individual can no longer remember basic social and survival skills or function independently. Language, spatial or temporal orientation, judgment, or other cognitive capacities may decline, and personality changes may also occur. Dementia is also present in other degenerative brain diseases including Pick disease and Parkinson disease.
The second most common cause of dementia is hypertension (high blood pressure) or other vascular conditions. This type of dementia, called multi-infarct, or vascular, dementia results from a series of small strokes that progressively destroy the brain. Dementia can also be caused by Huntington disease, syphilis, multiple sclerosis, acquired immune deficiency syndrome (AIDS), and some types of encephalitis. Treatable dementias occur in hypothyroidism, other metabolic diseases, and some malignant tumours. Treatment of the underlying disease in these cases may inhibit the progress of dementia but usually does not reverse it.
Pick disease
form of premature dementia caused by atrophy of the frontal and temporal lobes of the brain. It resembles Alzheimer disease but is much less common. Pick disease is characterized by a progressive deterioration of intellect, judgment, and memory, resulting in increased irritability, inappropriate behaviour, depression, and paranoia. Histologically some cerebral nerve cells are swollen and contain abnormal inclusions called Pick bodies. The cause of Pick disease is unknown, but in some cases the disease appears to be inherited. Average survival from onset (generally between the ages of 40 and 60) to death is about 10 years; there is no specific treatment. The disease was first described by the German neurologist Arnold Pick.
Hodgkin disease
an uncommon cancer of the lymphatic system (malignant lymphoma) that usually strikes young adults and people 55 years of age or older. Most patients can be cured if the disease is detected in its early stages, but even those with advanced Hodgkin disease have a significant chance of recovery. The overall cure rate is approximately 75 percent.
In its early stages the disease is characterized by local, painless swelling of one or more lymph nodes and sometimes by swelling of the spleen, liver, or other organs. In addition to swollen lymph nodes, symptoms may include fever and itching followed later by weight loss and fatigue. A microscopic examination of affected tissue, usually obtained from a lymph node, is required to confirm diagnosis.
The cause of Hodgkin disease remains unknown, but numerous infectious agents, including bacteria, protozoa, and viruses, have been suggested. Previous infection with the Epstein-Barr virus, the causative agent of mononucleosis, has been linked to many cases of Hodgkin disease. Hodgkin disease tumours develop from B lymphocytes. Treatment consists of chemotherapy, radiation, or a combination of both, depending on the stage of development of the disease.
The disease is named after Thomas Hodgkin, who first described it in 1832.
In its early stages the disease is characterized by local, painless swelling of one or more lymph nodes and sometimes by swelling of the spleen, liver, or other organs. In addition to swollen lymph nodes, symptoms may include fever and itching followed later by weight loss and fatigue. A microscopic examination of affected tissue, usually obtained from a lymph node, is required to confirm diagnosis.
The cause of Hodgkin disease remains unknown, but numerous infectious agents, including bacteria, protozoa, and viruses, have been suggested. Previous infection with the Epstein-Barr virus, the causative agent of mononucleosis, has been linked to many cases of Hodgkin disease. Hodgkin disease tumours develop from B lymphocytes. Treatment consists of chemotherapy, radiation, or a combination of both, depending on the stage of development of the disease.
The disease is named after Thomas Hodgkin, who first described it in 1832.
Monday, February 25, 2008
Mesothelioma
Mesothelioma is a form of cancer that is almost always caused by previous exposure to asbestos.[1] In this disease, malignant cells develop in the mesothelium, a protective lining that covers most of the body's internal organs. Its most common site is the pleura (outer lining of the lungs and chest cavity), but it may also occur in the peritoneum (the lining of the abdominal cavity) or the pericardium (a sac that surrounds the heart).
Most people who develop mesothelioma have worked on jobs where they inhaled asbestos particles, or have been exposed to asbestos dust and fibre in other ways, such as by washing the clothes of a family member who worked with asbestos, or by home renovation using asbestos cement products. Unlike lung cancer, there is no association between mesothelioma and smoking.
Signs and symptoms
Symptoms of mesothelioma may not appear until 20 to 50 years after exposure to asbestos. Shortness of breath, cough, and pain in the chest due to an accumulation of fluid in the pleural space are often symptoms of pleural mesothelioma.
Symptoms of peritoneal mesothelioma include weight loss and cachexia, abdominal swelling and pain due to ascites (a buildup of fluid in the abdominal cavity). Other symptoms of peritoneal mesothelioma may include bowel obstruction, blood clotting abnormalities, anemia, and fever. If the cancer has spread beyond the mesothelium to other parts of the body, symptoms may include pain, trouble swallowing, or swelling of the neck or face.
These symptoms may be caused by mesothelioma or by other, less serious conditions.
Mesothelioma that affects the pleura can cause these signs and symptoms:
* chest wall pain
* pleural effusion, or fluid surrounding the lung
* shortness of breath
* fatigue or anemia
* wheezing, hoarseness, or cough
* blood in the sputum (fluid) coughed up
In severe cases, the person may have many tumor masses. The individual may develop a pneumothorax, or collapse of the lung. The disease may metastasize, or spread, to other parts of the body.
Tumors that affect the abdominal cavity often do not cause symptoms until they are at a late stage. Symptoms include:
* abdominal pain
* ascites, or an abnormal buildup of fluid in the abdomen
* a mass in the abdomen
* problems with bowel function
* weight loss
In severe cases of the disease, the following signs and symptoms may be present:
* blood clots in the veins, which may cause thrombophlebitis
* disseminated intravascular coagulation, a disorder causing severe bleeding in many body organs
* jaundice, or yellowing of the eyes and skin
* low blood sugar level
* pleural effusion
* pulmonary emboli, or blood clots in the arteries of the lungs
* severe ascites
A mesothelioma does not usually spread to the bone, brain, or adrenal glands. Pleural tumors are usually found only on one side of the lungs.
Diagnosis
Diagnosing mesothelioma is often difficult, because the symptoms are similar to those of a number of other conditions. Diagnosis begins with a review of the patient's medical history. A history of exposure to asbestos may increase clinical suspicion for mesothelioma. A physical examination is performed, followed by chest X-ray and often lung function tests. The X-ray may reveal pleural thickening commonly seen after asbestos exposure and increases suspicion of mesothelioma. A CT (or CAT) scan or an MRI is usually performed. If a large amount of fluid is present, abnormal cells may be detected by cytology if this fluid is aspirated with a syringe. For pleural fluid this is done by a pleural tap or chest drain, in ascites with an paracentesis or ascitic drain and in a pericardial effusion with pericardiocentesis. While absence of malignant cells on cytology does not completely exclude mesothelioma, it makes it much more unlikely, especially if an alternative diagnosis can be made (e.g. tuberculosis, heart failure).
If cytology is positive or a plaque is regarded as suspicious, a biopsy is needed to confirm a diagnosis of mesothelioma. A doctor removes a sample of tissue for examination under a microscope by a pathologist. A biopsy may be done in different ways, depending on where the abnormal area is located. If the cancer is in the chest, the doctor may perform a thoracoscopy. In this procedure, the doctor makes a small cut through the chest wall and puts a thin, lighted tube called a thoracoscope into the chest between two ribs. Thoracoscopy allows the doctor to look inside the chest and obtain tissue samples.
If the cancer is in the abdomen, the doctor may perform a laparoscopy. To obtain tissue for examination, the doctor makes a small opening in the abdomen and inserts a special instrument into the abdominal cavity. If these procedures do not yield enough tissue, more extensive diagnostic surgery may be necessary.
Doctors have begun testing the Mesomark assay which measures levels of soluble mesothelin-related proteins (SMRPs) released by diseased mesothelioma cells. The procedure could diagnose mesothelioma earlier than conventional methods thus improving the survival prospects for patients
Treatment
Treatment of MM using conventional therapies has not proved successful and patients have a median survival time of 6 - 12 months after presentation[citation needed]. The clinical behaviour of the malignancy is affected by several factors including the continuous mesothelial surface of the pleural cavity which favours local metastasis via exfoliated cells, invasion to underlying tissue and other organs within the pleural cavity, and the extremely long latency period between asbestos exposure and development of the disease.
Surgery
Surgery, either by itself or used in combination with pre- and post-operative adjuvant therapies, has proved disappointing. A pleurectomy/decortication is the most common surgery, in which the lining of the chest is removed. Less common is an extrapleural pneumonectomy (EPP), in which the lung, lining of the inside of the chest, the hemi-diaphragm and the pericardium are removed. It is not possible to remove the entire mesothelium without killing the patient.
Radiation
For patients with localized disease, and who can tolerate a radical surgery, radiation is often given post-operatively as a consolidative treatment. The entire hemi-thorax is treated with radiation therapy, often given simultaneously with chemotherapy. This approach of using surgery followed by radiation with chemotherapy has been pioneered by the thoracic oncology team at Brigham & Women's Hospital in Boston.Delivering radiation and chemotherapy after a radical surgery has led to extended life expectancy in selected patient populations with some patients surviving more than 5 years. As part of a curative approach to mesothelioma, radiotherapy is also commonly applied to the sites of chest drain insertion, in order to prevent growth of the tumor along the track in the chest wall.
Although mesothelioma is generally resistant to curative treatment with radiotherapy alone, palliative treatment regimens are sometimes used to relieve symptoms arising from tumor growth, such as obstruction of a major blood vessel. Radiation therapy when given alone with curative intent has never been shown to improve survival from mesothelioma. The necessary radiation dose to treat mesothelioma that has not been surgically removed would be very toxic.
Chemotherapy
In February 2004, the United States Food and Drug Administration approved pemetrexed (brand name Alimta) for treatment of malignant pleural mesothelioma. Pemetrexed is given in combination with cisplatin. Folic acid is also used to reduce the side-effects of pemetrexed.
Immunotherapy
Treatment regimens involving immunotherapy have yielded variable results. For example, intrapleural inoculation of Bacillus Calmette-Guérin (BCG) in an attempt to boost the immune response, was found to be of no benefit to the patient (while it may benefit patients with bladder cancer). Mesothelioma cells proved susceptible to in vitro lysis by LAK cells following activation by interleukin-2 (IL-2), but patients undergoing this particular therapy experienced major side effects. Indeed, this trial was suspended in view of the unacceptably high levels of IL-2 toxicity and the severity of side effects such as fever and cachexia. Nonetheless, other trials involving interferon alpha have proved more encouraging with 20% of patients experiencing a greater than 50% reduction in tumor mass combined with minimal side effects.
Heated Intraoperative Intraperitoneal Chemotherapy
A procedure known as heated intraoperative intraperitoneal chemotherapy was developed by Paul Sugarbaker at the Washington Cancer Institute.The surgeon removes as much of the tumor as possible followed by the direct administration of a chemotherapy agent, heated to between 40 and 48°C, in the abdomen. The fluid is perfused for 60 to 120 minutes and then drained.
This technique permits the administration of high concentrations of selected drugs into the abdominal and pelvic surfaces. Heating the chemotherapy treatment increases the penetration of the drugs into tissues. Also, heating itself damages the malignant cells more than the normal cells.
Most people who develop mesothelioma have worked on jobs where they inhaled asbestos particles, or have been exposed to asbestos dust and fibre in other ways, such as by washing the clothes of a family member who worked with asbestos, or by home renovation using asbestos cement products. Unlike lung cancer, there is no association between mesothelioma and smoking.
Signs and symptoms
Symptoms of mesothelioma may not appear until 20 to 50 years after exposure to asbestos. Shortness of breath, cough, and pain in the chest due to an accumulation of fluid in the pleural space are often symptoms of pleural mesothelioma.
Symptoms of peritoneal mesothelioma include weight loss and cachexia, abdominal swelling and pain due to ascites (a buildup of fluid in the abdominal cavity). Other symptoms of peritoneal mesothelioma may include bowel obstruction, blood clotting abnormalities, anemia, and fever. If the cancer has spread beyond the mesothelium to other parts of the body, symptoms may include pain, trouble swallowing, or swelling of the neck or face.
These symptoms may be caused by mesothelioma or by other, less serious conditions.
Mesothelioma that affects the pleura can cause these signs and symptoms:
* chest wall pain
* pleural effusion, or fluid surrounding the lung
* shortness of breath
* fatigue or anemia
* wheezing, hoarseness, or cough
* blood in the sputum (fluid) coughed up
In severe cases, the person may have many tumor masses. The individual may develop a pneumothorax, or collapse of the lung. The disease may metastasize, or spread, to other parts of the body.
Tumors that affect the abdominal cavity often do not cause symptoms until they are at a late stage. Symptoms include:
* abdominal pain
* ascites, or an abnormal buildup of fluid in the abdomen
* a mass in the abdomen
* problems with bowel function
* weight loss
In severe cases of the disease, the following signs and symptoms may be present:
* blood clots in the veins, which may cause thrombophlebitis
* disseminated intravascular coagulation, a disorder causing severe bleeding in many body organs
* jaundice, or yellowing of the eyes and skin
* low blood sugar level
* pleural effusion
* pulmonary emboli, or blood clots in the arteries of the lungs
* severe ascites
A mesothelioma does not usually spread to the bone, brain, or adrenal glands. Pleural tumors are usually found only on one side of the lungs.
Diagnosis
Diagnosing mesothelioma is often difficult, because the symptoms are similar to those of a number of other conditions. Diagnosis begins with a review of the patient's medical history. A history of exposure to asbestos may increase clinical suspicion for mesothelioma. A physical examination is performed, followed by chest X-ray and often lung function tests. The X-ray may reveal pleural thickening commonly seen after asbestos exposure and increases suspicion of mesothelioma. A CT (or CAT) scan or an MRI is usually performed. If a large amount of fluid is present, abnormal cells may be detected by cytology if this fluid is aspirated with a syringe. For pleural fluid this is done by a pleural tap or chest drain, in ascites with an paracentesis or ascitic drain and in a pericardial effusion with pericardiocentesis. While absence of malignant cells on cytology does not completely exclude mesothelioma, it makes it much more unlikely, especially if an alternative diagnosis can be made (e.g. tuberculosis, heart failure).
If cytology is positive or a plaque is regarded as suspicious, a biopsy is needed to confirm a diagnosis of mesothelioma. A doctor removes a sample of tissue for examination under a microscope by a pathologist. A biopsy may be done in different ways, depending on where the abnormal area is located. If the cancer is in the chest, the doctor may perform a thoracoscopy. In this procedure, the doctor makes a small cut through the chest wall and puts a thin, lighted tube called a thoracoscope into the chest between two ribs. Thoracoscopy allows the doctor to look inside the chest and obtain tissue samples.
If the cancer is in the abdomen, the doctor may perform a laparoscopy. To obtain tissue for examination, the doctor makes a small opening in the abdomen and inserts a special instrument into the abdominal cavity. If these procedures do not yield enough tissue, more extensive diagnostic surgery may be necessary.
Doctors have begun testing the Mesomark assay which measures levels of soluble mesothelin-related proteins (SMRPs) released by diseased mesothelioma cells. The procedure could diagnose mesothelioma earlier than conventional methods thus improving the survival prospects for patients
Treatment
Treatment of MM using conventional therapies has not proved successful and patients have a median survival time of 6 - 12 months after presentation[citation needed]. The clinical behaviour of the malignancy is affected by several factors including the continuous mesothelial surface of the pleural cavity which favours local metastasis via exfoliated cells, invasion to underlying tissue and other organs within the pleural cavity, and the extremely long latency period between asbestos exposure and development of the disease.
Surgery
Surgery, either by itself or used in combination with pre- and post-operative adjuvant therapies, has proved disappointing. A pleurectomy/decortication is the most common surgery, in which the lining of the chest is removed. Less common is an extrapleural pneumonectomy (EPP), in which the lung, lining of the inside of the chest, the hemi-diaphragm and the pericardium are removed. It is not possible to remove the entire mesothelium without killing the patient.
Radiation
For patients with localized disease, and who can tolerate a radical surgery, radiation is often given post-operatively as a consolidative treatment. The entire hemi-thorax is treated with radiation therapy, often given simultaneously with chemotherapy. This approach of using surgery followed by radiation with chemotherapy has been pioneered by the thoracic oncology team at Brigham & Women's Hospital in Boston.Delivering radiation and chemotherapy after a radical surgery has led to extended life expectancy in selected patient populations with some patients surviving more than 5 years. As part of a curative approach to mesothelioma, radiotherapy is also commonly applied to the sites of chest drain insertion, in order to prevent growth of the tumor along the track in the chest wall.
Although mesothelioma is generally resistant to curative treatment with radiotherapy alone, palliative treatment regimens are sometimes used to relieve symptoms arising from tumor growth, such as obstruction of a major blood vessel. Radiation therapy when given alone with curative intent has never been shown to improve survival from mesothelioma. The necessary radiation dose to treat mesothelioma that has not been surgically removed would be very toxic.
Chemotherapy
In February 2004, the United States Food and Drug Administration approved pemetrexed (brand name Alimta) for treatment of malignant pleural mesothelioma. Pemetrexed is given in combination with cisplatin. Folic acid is also used to reduce the side-effects of pemetrexed.
Immunotherapy
Treatment regimens involving immunotherapy have yielded variable results. For example, intrapleural inoculation of Bacillus Calmette-Guérin (BCG) in an attempt to boost the immune response, was found to be of no benefit to the patient (while it may benefit patients with bladder cancer). Mesothelioma cells proved susceptible to in vitro lysis by LAK cells following activation by interleukin-2 (IL-2), but patients undergoing this particular therapy experienced major side effects. Indeed, this trial was suspended in view of the unacceptably high levels of IL-2 toxicity and the severity of side effects such as fever and cachexia. Nonetheless, other trials involving interferon alpha have proved more encouraging with 20% of patients experiencing a greater than 50% reduction in tumor mass combined with minimal side effects.
Heated Intraoperative Intraperitoneal Chemotherapy
A procedure known as heated intraoperative intraperitoneal chemotherapy was developed by Paul Sugarbaker at the Washington Cancer Institute.The surgeon removes as much of the tumor as possible followed by the direct administration of a chemotherapy agent, heated to between 40 and 48°C, in the abdomen. The fluid is perfused for 60 to 120 minutes and then drained.
This technique permits the administration of high concentrations of selected drugs into the abdominal and pelvic surfaces. Heating the chemotherapy treatment increases the penetration of the drugs into tissues. Also, heating itself damages the malignant cells more than the normal cells.
Saturday, February 23, 2008
Haemophilia
Haemophilia or hemophilia (from Greek haima "blood" and philia "to love") is the name of a family of hereditary genetic disorders that impair the body's ability to control blood clotting, or coagulation. In the most common form, hemophilia A, clotting factor VIII is absent. Haemophilia B, also known as factor IX deficiency, is the second most common type of hemophilia, but Hemophilia B is far less common than Hemophilia A, the latter occurring in about one in 25,000 male births.
The effects of this sex-linked, X chromosome disorder are manifested almost entirely in males, although the gene for the disorder is inherited from the mother. This is more common in males because the female has two X chromosomes while the male only has one, meaning that if a male's x chromosome is defective, there is not another to "cover up" the disorder like females have. Sometimes this disease is considered to be dominant because of its dominance in the male XY chromosome pair. In about 30% of cases of Hemopilia B, however, there is no family history of the disorder and the condition is the result of a spontaneous gene mutation. A mother who is a carrier also has a 50% chance of giving the faulty X chromosome to her daughter. That does not give the daughter the hemophilia disease, but it does result in the daughter becoming a hemophilia carrier. Females are almost exclusively asymptomatic carriers of the disorder, and may have inherited it from either their mother or father.
These genetic deficiencies may lower blood plasma clotting factor levels of coagulation factors needed for a normal clotting process. When a blood vessel is injured, a temporary scab does form, but the missing coagulation factors prevent fibrin formation which is necessary to maintain the blood clot. Thus a haemophiliac does not bleed more intensely than a normal person, but for a much longer amount of time. In severe haemophiliacs even a minor injury could result in blood loss lasting days, weeks, or not ever healing completely. The critical risk here is with normally small bleeds which due to missing factor VIII take long times to heal. In areas such as the brain or inside joints this can be fatal or life debilitating.
The bleeding with external injury is normal, but incidence of late re-bleeding and internal bleeding is increased, especially into muscles, joints, or bleeding into closed spaces. Major complications include hemarthrosis, hemorrhage, gastrointestinal bleeding, and menorrhagia.
Causes
It is caused by a lack of clotting factors:
* Hemophilia A involves a lack of functional clotting Factor VIII. (This represents 90% of haemophilia cases.[citation needed])
* Hemophilia B involves a lack of functional clotting Factor IX.
* Hemophilia C involves a lack of functional clotting Factor XI.
* Hypofibrinogenemia involves a lack of functional clotting factor Factor I. Because it is so rare, about 1 or 2 cases per million births, it has no definite treatment approved by the FDA. It affects males and females equally. The blood of people with Hypofibrinogenemia neither clots nor contains sufficient amounts of Fibrinogen.
History
The earliest possible implicit reference to hemophilia may have been in the Talmud[4], a Jewish holy text, which states that males did not have to be circumcised if two brothers had already died from the procedure. In 1000, the Arab physician Abu al-Qasim al-Zahrawi (known as Albucasis in the West) wrote a more explicit description of hemophilia in his Al-Tasrif, in which he wrote of an Andalusian family whose males died of bleeding after minor injuries.
In 1803, Dr. John Conrad Otto, a Philadelphia physician, wrote an account about "a hemorrhagic disposition existing in certain families." He recognized that the disorder was hereditary and that it affected males and rarely females. He was able to trace the disease back to a woman who settled near Plymouth in 1720. The first usage of the term "hemophilia" appears in a description of the condition written by Hopff at the University of Zurich in 1828. In 1937, Patek and Taylor, two doctors from Harvard, discovered anti-hemophilic globulin. Pavlosky, a doctor from Buenos Aires, found Hemophilia A and Hemophilia B to be separate diseases by doing a lab test. This test was done by transferring the blood of one hemophiliac to another hemophiliac. The fact that this corrected the clotting problem showed that there was more than one form of hemophilia.
Haemophilia in European royalty featured prominently and thus is sometimes known as "the royal disease". Queen Victoria passed the mutation to her son Leopold and, through several of her daughters, to various royals across the continent, including the royal families of Spain, Germany, and Russia. Tsarevich Alexei Nikolaevich, son of Nicholas II, was a descendant of Queen Victoria and suffered from hemophilia.
Prior to 1985, there were no laws enacted within the U.S. to screen blood, even though the technology existed. As a result, many hemophilia patients who received untested and unscreened clotting factor prior to 1992 were at an extreme risk for contracting HIV and Hepatitis C via these blood products. It is estimated that more than 50% of the Hemophilia population, over 10,000 people, contracted HIV from the tainted blood supply in the United States alone.
About 18,000 people in the United States have hemophilia. Each year, about 400 babies are born with the disorder. Hemophilia usually occurs in males and less often in females.
Genetics
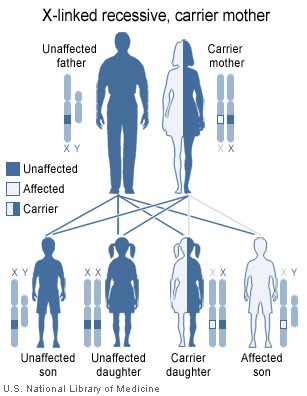
Females possess two X-chromosomes, whereas males have one X and one Y chromosome. Since the mutations causing the disease are recessive, a woman carrying the defect on one of her X-chromosomes may not be affected by it, as the equivalent allele on her other chromosome should express itself to produce the necessary clotting factors. However the Y-chromosome in men has no gene for factors VIII or IX. If the genes responsible for production of factor VIII or factor IX present on a male's X-chromosome are deficient there is no equivalent on the Y-chromosome, so the deficient gene is not masked by the dominant allele and he will develop the illness.
Since a male receives his single X-chromosome from his mother, the son of a healthy female silently carrying the deficient gene will have a 50% chance of inheriting that gene from her and with it the disease; and if his mother is affected with haemophilia, he will have a 100% chance of being a haemophiliac. In contrast, for a female to inherit the disease, she must receive two deficient X-chromosomes, one from her mother and the other from her father (who must therefore be a haemophiliac himself). Hence haemophilia is far more common among males than females. However it is possible for female carriers to become mild haemophiliacs due to lyonisation of the X chromosomes. Haemophiliac daughters are more common than they once were, as improved treatments for the disease have allowed more haemophiliac males to survive to adulthood and become parents. Adult females may experience menorrhagia (heavy periods) due to the bleeding tendency. The pattern of inheritance is criss-cross type. This type of pattern is also seen in colour blindness.
As with all genetic disorders, it is of course also possible for a human to acquire it spontaneously through mutation, rather than inheriting it, because of a new mutation in one of their parents' gametes. Spontaneous mutations account for about ⅓ of all haemophilia A and 20% of all hemophilia B cases. Genetic testing and genetic counseling is recommended for families with haemophilia. Prenatal testing, such as amniocentesis, is available to pregnant women who may be carriers of the condition.
Treatment
Though there is no cure for hemophilia, it can be controlled with regular infusions of the deficient clotting factor, i.e. factor VIII in haemophilia A or factor IX in hemophilia B. Some hemophiliacs develop antibodies (inhibitors) against the replacement factors given to them, so the amount of the factor has to be increased or non-human replacement products must be given, such as porcine factor VIII.
If a patient becomes refractory to replacement coagulation factor as a result of circulating inhibitors, this may be partially overcome with recombinant human factor VII (NovoSeven®), which is registered for this indication in many countries.
In early 2008, the US Food and Drug Administration approved Xyntha® (Wyeth) anti-hemophilic factor, genetically engineered from the genes of Chinese hamster ovary cells. Since 1993 (Dr. Mary Nugent) recombinant factor products (which are typically cultured in Chinese hamster ovary (CHO) tissue culture cells and involve little, if any human plasma products) have been available and have been widely used in wealthier western countries. While recombinant clotting factor products offer higher purity and safety, they are, like concentrate, extremely expensive, and not generally available in the developing world. In many cases, factor products of any sort are difficult to obtain in developing countries.
In Western countries, common standards of care fall into one of two categories: prophylaxis or on-demand. Prophylaxis involves the infusion of clotting factor on a regular schedule in order to keep clotting levels sufficiently high to prevent spontaneous bleeding episodes. On-demand treatment involves treating bleeding episodes once they arise. In 2007, a clinical trial was published in the New England Journal of Medicine (NEJM) comparing on-demand treatment of boys (< 30 months) with Hemophilia A with prophylactic treatment (infusions of 25 IU/kg body weight of Factor VIII every other day) in respect to its effect on the prevention of joint-diseases. When the boys reached 6 years of age, 93% of those in the prophylaxis group and 55% of those in the episodic-therapy group had a normal index joint-structure on MRI. Prophylactic treatment, however, resulted in average costs of $300,000 per year. The author of an editorial published in the same issue of the NEJM demands more clinical studies addressing the cost-effectiveness of prophylactic treatment.
Armour and other pharmaceutical companies knowingly sold blood clotting products contaminated with HIV and hepatitis C to ten thousand hemophiliacs across America in the late 1970's and early mid 1980's. When the Federal Government banned their products from being sold in America, they promptly turned around and sold the HIV contaminated factor products overseas in Europe and Japan.
Later criminal and civil lawsuits were brought against these manufacturers and the Armour Pharmaceutical subsidiary of French chemical company Rhone-Poulenc. In Europe and Japan several high level executives received prison terms as a result of their knowingly selling HIV contaminated products to hemophiliacs.
In America the pharmaceutical companies eventually paid out around 650 million dollars to compensate the haemophiliacs who were infected with HIV. [12]
As a direct result of the contamination of the blood supply in the late 1970s and early/mid 1980s with viruses such as Hepatitis and HIV, new methods were developed in the production of clotting factor products. The initial response was to heat-treat (pasteurize) plasma-derived factor concentrate, followed by the development of monoclonal factor concentrates, which use a combination of heat treatment and affinity chromatography to inactivate any viral agents in the pooled plasma from which the factor concentrate is derived. The Lindsay Tribunal in Ireland investigated, among other things, the slow adoption of the new methods.
It was claimed that Rasputin was successful at treating the Tsarevich Alexei of Russia's hemophilia. At the time, a common treatment administered by professional doctors was to use aspirin, which worsened rather than lessen the problem. It is believe that, by simply advising against the medical treatment, Rasputin could bring visible and significant improvement to the condition of Alexei.
People affected with Hemophilia are recommended to do some specific exercises for elbow, knee, and ankles like stretching of calves, ankle circles, elbow flexion, and Quadriceps set etc. These exercises are recommended after an internal bleed occurs and on a daily basis to strengthen the muscles and joints to prevent new bleeding problems.
The effects of this sex-linked, X chromosome disorder are manifested almost entirely in males, although the gene for the disorder is inherited from the mother. This is more common in males because the female has two X chromosomes while the male only has one, meaning that if a male's x chromosome is defective, there is not another to "cover up" the disorder like females have. Sometimes this disease is considered to be dominant because of its dominance in the male XY chromosome pair. In about 30% of cases of Hemopilia B, however, there is no family history of the disorder and the condition is the result of a spontaneous gene mutation. A mother who is a carrier also has a 50% chance of giving the faulty X chromosome to her daughter. That does not give the daughter the hemophilia disease, but it does result in the daughter becoming a hemophilia carrier. Females are almost exclusively asymptomatic carriers of the disorder, and may have inherited it from either their mother or father.
These genetic deficiencies may lower blood plasma clotting factor levels of coagulation factors needed for a normal clotting process. When a blood vessel is injured, a temporary scab does form, but the missing coagulation factors prevent fibrin formation which is necessary to maintain the blood clot. Thus a haemophiliac does not bleed more intensely than a normal person, but for a much longer amount of time. In severe haemophiliacs even a minor injury could result in blood loss lasting days, weeks, or not ever healing completely. The critical risk here is with normally small bleeds which due to missing factor VIII take long times to heal. In areas such as the brain or inside joints this can be fatal or life debilitating.
The bleeding with external injury is normal, but incidence of late re-bleeding and internal bleeding is increased, especially into muscles, joints, or bleeding into closed spaces. Major complications include hemarthrosis, hemorrhage, gastrointestinal bleeding, and menorrhagia.
Causes
It is caused by a lack of clotting factors:
* Hemophilia A involves a lack of functional clotting Factor VIII. (This represents 90% of haemophilia cases.[citation needed])
* Hemophilia B involves a lack of functional clotting Factor IX.
* Hemophilia C involves a lack of functional clotting Factor XI.
* Hypofibrinogenemia involves a lack of functional clotting factor Factor I. Because it is so rare, about 1 or 2 cases per million births, it has no definite treatment approved by the FDA. It affects males and females equally. The blood of people with Hypofibrinogenemia neither clots nor contains sufficient amounts of Fibrinogen.
History
The earliest possible implicit reference to hemophilia may have been in the Talmud[4], a Jewish holy text, which states that males did not have to be circumcised if two brothers had already died from the procedure. In 1000, the Arab physician Abu al-Qasim al-Zahrawi (known as Albucasis in the West) wrote a more explicit description of hemophilia in his Al-Tasrif, in which he wrote of an Andalusian family whose males died of bleeding after minor injuries.
In 1803, Dr. John Conrad Otto, a Philadelphia physician, wrote an account about "a hemorrhagic disposition existing in certain families." He recognized that the disorder was hereditary and that it affected males and rarely females. He was able to trace the disease back to a woman who settled near Plymouth in 1720. The first usage of the term "hemophilia" appears in a description of the condition written by Hopff at the University of Zurich in 1828. In 1937, Patek and Taylor, two doctors from Harvard, discovered anti-hemophilic globulin. Pavlosky, a doctor from Buenos Aires, found Hemophilia A and Hemophilia B to be separate diseases by doing a lab test. This test was done by transferring the blood of one hemophiliac to another hemophiliac. The fact that this corrected the clotting problem showed that there was more than one form of hemophilia.
Haemophilia in European royalty featured prominently and thus is sometimes known as "the royal disease". Queen Victoria passed the mutation to her son Leopold and, through several of her daughters, to various royals across the continent, including the royal families of Spain, Germany, and Russia. Tsarevich Alexei Nikolaevich, son of Nicholas II, was a descendant of Queen Victoria and suffered from hemophilia.
Prior to 1985, there were no laws enacted within the U.S. to screen blood, even though the technology existed. As a result, many hemophilia patients who received untested and unscreened clotting factor prior to 1992 were at an extreme risk for contracting HIV and Hepatitis C via these blood products. It is estimated that more than 50% of the Hemophilia population, over 10,000 people, contracted HIV from the tainted blood supply in the United States alone.
About 18,000 people in the United States have hemophilia. Each year, about 400 babies are born with the disorder. Hemophilia usually occurs in males and less often in females.
Genetics
Females possess two X-chromosomes, whereas males have one X and one Y chromosome. Since the mutations causing the disease are recessive, a woman carrying the defect on one of her X-chromosomes may not be affected by it, as the equivalent allele on her other chromosome should express itself to produce the necessary clotting factors. However the Y-chromosome in men has no gene for factors VIII or IX. If the genes responsible for production of factor VIII or factor IX present on a male's X-chromosome are deficient there is no equivalent on the Y-chromosome, so the deficient gene is not masked by the dominant allele and he will develop the illness.
Since a male receives his single X-chromosome from his mother, the son of a healthy female silently carrying the deficient gene will have a 50% chance of inheriting that gene from her and with it the disease; and if his mother is affected with haemophilia, he will have a 100% chance of being a haemophiliac. In contrast, for a female to inherit the disease, she must receive two deficient X-chromosomes, one from her mother and the other from her father (who must therefore be a haemophiliac himself). Hence haemophilia is far more common among males than females. However it is possible for female carriers to become mild haemophiliacs due to lyonisation of the X chromosomes. Haemophiliac daughters are more common than they once were, as improved treatments for the disease have allowed more haemophiliac males to survive to adulthood and become parents. Adult females may experience menorrhagia (heavy periods) due to the bleeding tendency. The pattern of inheritance is criss-cross type. This type of pattern is also seen in colour blindness.
As with all genetic disorders, it is of course also possible for a human to acquire it spontaneously through mutation, rather than inheriting it, because of a new mutation in one of their parents' gametes. Spontaneous mutations account for about ⅓ of all haemophilia A and 20% of all hemophilia B cases. Genetic testing and genetic counseling is recommended for families with haemophilia. Prenatal testing, such as amniocentesis, is available to pregnant women who may be carriers of the condition.
Treatment
Though there is no cure for hemophilia, it can be controlled with regular infusions of the deficient clotting factor, i.e. factor VIII in haemophilia A or factor IX in hemophilia B. Some hemophiliacs develop antibodies (inhibitors) against the replacement factors given to them, so the amount of the factor has to be increased or non-human replacement products must be given, such as porcine factor VIII.
If a patient becomes refractory to replacement coagulation factor as a result of circulating inhibitors, this may be partially overcome with recombinant human factor VII (NovoSeven®), which is registered for this indication in many countries.
In early 2008, the US Food and Drug Administration approved Xyntha® (Wyeth) anti-hemophilic factor, genetically engineered from the genes of Chinese hamster ovary cells. Since 1993 (Dr. Mary Nugent) recombinant factor products (which are typically cultured in Chinese hamster ovary (CHO) tissue culture cells and involve little, if any human plasma products) have been available and have been widely used in wealthier western countries. While recombinant clotting factor products offer higher purity and safety, they are, like concentrate, extremely expensive, and not generally available in the developing world. In many cases, factor products of any sort are difficult to obtain in developing countries.
In Western countries, common standards of care fall into one of two categories: prophylaxis or on-demand. Prophylaxis involves the infusion of clotting factor on a regular schedule in order to keep clotting levels sufficiently high to prevent spontaneous bleeding episodes. On-demand treatment involves treating bleeding episodes once they arise. In 2007, a clinical trial was published in the New England Journal of Medicine (NEJM) comparing on-demand treatment of boys (< 30 months) with Hemophilia A with prophylactic treatment (infusions of 25 IU/kg body weight of Factor VIII every other day) in respect to its effect on the prevention of joint-diseases. When the boys reached 6 years of age, 93% of those in the prophylaxis group and 55% of those in the episodic-therapy group had a normal index joint-structure on MRI. Prophylactic treatment, however, resulted in average costs of $300,000 per year. The author of an editorial published in the same issue of the NEJM demands more clinical studies addressing the cost-effectiveness of prophylactic treatment.
Armour and other pharmaceutical companies knowingly sold blood clotting products contaminated with HIV and hepatitis C to ten thousand hemophiliacs across America in the late 1970's and early mid 1980's. When the Federal Government banned their products from being sold in America, they promptly turned around and sold the HIV contaminated factor products overseas in Europe and Japan.
Later criminal and civil lawsuits were brought against these manufacturers and the Armour Pharmaceutical subsidiary of French chemical company Rhone-Poulenc. In Europe and Japan several high level executives received prison terms as a result of their knowingly selling HIV contaminated products to hemophiliacs.
In America the pharmaceutical companies eventually paid out around 650 million dollars to compensate the haemophiliacs who were infected with HIV. [12]
As a direct result of the contamination of the blood supply in the late 1970s and early/mid 1980s with viruses such as Hepatitis and HIV, new methods were developed in the production of clotting factor products. The initial response was to heat-treat (pasteurize) plasma-derived factor concentrate, followed by the development of monoclonal factor concentrates, which use a combination of heat treatment and affinity chromatography to inactivate any viral agents in the pooled plasma from which the factor concentrate is derived. The Lindsay Tribunal in Ireland investigated, among other things, the slow adoption of the new methods.
It was claimed that Rasputin was successful at treating the Tsarevich Alexei of Russia's hemophilia. At the time, a common treatment administered by professional doctors was to use aspirin, which worsened rather than lessen the problem. It is believe that, by simply advising against the medical treatment, Rasputin could bring visible and significant improvement to the condition of Alexei.
People affected with Hemophilia are recommended to do some specific exercises for elbow, knee, and ankles like stretching of calves, ankle circles, elbow flexion, and Quadriceps set etc. These exercises are recommended after an internal bleed occurs and on a daily basis to strengthen the muscles and joints to prevent new bleeding problems.
Hepatitis

Hepatitis (plural hepatitides) implies injury to liver characterised by presence of inflammatory cells in the liver tissue. Etymologically from ancient Greek hepar (ηπαρ) or hepato- (ηπατο-) meaning 'liver' and suffix -itis denoting 'inflammation' (c.1727[1]). The condition can be self limiting, healing on its own or can progress to scarring of the liver. Hepatitis is acute when it lasts less than 6 months and chronic when it persists longer. A group of viruses known as the hepatitis viruses cause most cases of liver damage worldwide. Hepatitis can also be due to toxins (notably alcohol), other infections or from autoimmune process. It may run a subclinical course when the affected person may not feel ill. The patient becomes unwell and symptomatic when the disease impairs liver functions that include, among other things, screening of harmful substances, regulation of blood composition, and production of bile to help digestion.
Causes
Acute hepatitis
* Viral Hepatitis: Hepatitis A to E (more than 95% of viral cause), Herpes simplex, Cytomegalovirus, Epstein-Barr, yellow fever virus, adenoviruses.
* Non viral infection: toxoplasma, Leptospira, Q fever,[2] rocky mountain spotted fever[3]
* Alcohol
* Toxins: Amanita toxin in mushrooms, Carbon tetrachloride, asafetida
* Drugs: Paracetamol, amoxycillin, anti tuberculosis medicines, minocycline and many others (see longer list below).
* Ischemic hepatitis (circulatory insufficiency)
* Pregnancy
* Auto immune conditions e.g. Systemic Lupus Erythematosus (SLE)
* Metabolic diseases e.g. Wilson's disease
Chronic hepatitis
* Viral Hepatitis: Hepatitis B with or without hepatitis D, Hepatitis C (Hepatitis A and E do not lead to chronic disease)
* Autoimmune: Autoimmune hepatitis
* Alcohol
* Drugs: methyl-dopa, nitrofurantoin, isoniazide, ketoconazole
* Non-alcoholic steatohepatitis
* Heredity: Wilson's disease, alpha 1-antitrypsin deficiency
* Primary biliary cirrhosis and primary sclerosing cholangitis occasionally mimic chronic hepatitis
Signs and symptoms
Acute Hepatitis
Clinically, the course of acute hepatitis varies widely from mild symptoms requiring no treatment to fulminant hepatic failure needing liver transplantation. Acute viral hepatitis are more likely to be asymptomatic in younger people. Symptomatic individuals may present after convalescent stage of 7 to 10 days, with the total illness lasting 2 to 6 weeks.[4]
Initial features are of nonspecific flu-like symptoms, common to almost all acute viral infections and may include malaise, muscle and joint aches, fever, nausea or vomiting, diarrhea, and headache. More specific symptoms, which can be present in acute hepatitis from any cause are: profound loss of appetite, aversion to smoking among smokers, dark urine, yellowing of the eyes and skin (i.e. jaundice) and abdominal discomfort. Physical findings are usually minimal, apart from jaundice (33%) and tender hepatomegaly (10%). There can be occasional lymphadenopathy (5%) or splenomegaly (5%).[5]
Chronic Hepatitis
Majority of patients will remain asymptomatic or mildly symptomatic, abnormal blood tests being the only manifestation. Features may be related to extent of liver damage or the cause of hepatitis. Many experience return of symptoms related to acute hepatitis. Jaundice can be a late feature and may indicate extensive damage. Other features include abdominal fullness from enlarged liver or spleen, low grade fever and fluid retention (ascites). Extensive damage and scarring of liver i.e. cirrhosis leads to weight loss, easy bruising and bleeding tendencies. Acne, abnormal menstruation, lung scarring, inflammation of the thyroid gland and kidneys may be present in women with autoimmune hepatitis.[6]
Findings on clinical examination are usually those of cirrhosis or are related to aetiology.
AIDS

Acquired immune deficiency syndrome or acquired immunodeficiency syndrome (AIDS or Aids) is a collection of symptoms and infections resulting from the specific damage to the immune system caused by the human immunodeficiency virus (HIV) in humans,[1] and similar viruses in other species (SIV, FIV, etc.). The late stage of the condition leaves individuals susceptible to opportunistic infections and tumors. Although treatments for AIDS and HIV exist to decelerate the virus's progression, there is currently no known cure. HIV, et al., are transmitted through direct contact of a mucous membrane or the bloodstream with a bodily fluid containing HIV, such as blood, semen, vaginal fluid, preseminal fluid, and breast milk.[2][3] This transmission can come in the form of anal, vaginal or oral sex, blood transfusion, contaminated hypodermic needles, exchange between mother and baby during pregnancy, childbirth, or breastfeeding, or other exposure to one of the above bodily fluids.
Most researchers believe that HIV originated in sub-Saharan Africa during the twentieth century;[4] it is now a pandemic, with an estimated 33.2 million people now living with the disease worldwide.[5] As of January 2006, the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organization (WHO) estimate that AIDS has killed more than 25 million people since it was first recognized on June 5, 1981, making it one of the most destructive epidemics in recorded history. In 2005 alone, AIDS claimed an estimated 2.4–3.3 million lives, of which more than 570,000 were children.[6] A third of these deaths are occurring in sub-Saharan Africa, retarding economic growth and destroying human capital. Antiretroviral treatment reduces both the mortality and the morbidity of HIV infection, but routine access to antiretroviral medication is not available in all countries.[7] HIV/AIDS stigma is more severe than that associated with other life-threatening conditions and extends beyond the disease itself to providers and even volunteers involved with the care of people living with HIV.
Diagnosis
Since June 5, 1981, many definitions have been developed for epidemiological surveillance such as the Bangui definition and the 1994 expanded World Health Organization AIDS case definition. However, clinical staging of patients was not an intended use for these systems as they are neither sensitive, nor specific. In developing countries, the World Health Organization staging system for HIV infection and disease, using clinical and laboratory data, is used and in developed countries, the Centers for Disease Control (CDC) Classification System is used.
WHO disease staging system for HIV infection and disease
Main article: WHO Disease Staging System for HIV Infection and Disease
In 1990, the World Health Organization (WHO) grouped these infections and conditions together by introducing a staging system for patients infected with HIV-1.[21] An update took place in September 2005. Most of these conditions are opportunistic infections that are easily treatable in healthy people.
* Stage I: HIV infection is asymptomatic and not categorized as AIDS
* Stage II: includes minor mucocutaneous manifestations and recurrent upper respiratory tract infections
* Stage III: includes unexplained chronic diarrhea for longer than a month, severe bacterial infections and pulmonary tuberculosis
* Stage IV: includes toxoplasmosis of the brain, candidiasis of the esophagus, trachea, bronchi or lungs and Kaposi's sarcoma; these diseases are indicators of AIDS.
CDC classification system for HIV infection
Main article: CDC Classification System for HIV Infection
In the beginning, the Centers for Disease Control and Prevention (CDC) did not have an official name for the disease, often referring to it by way of the diseases that were associated with it, for example, lymphadenopathy, the disease after which the discoverers of HIV originally named the virus.[22][23] They also used Kaposi's Sarcoma and Opportunistic Infections, the name by which a task force had been set up in 1981.[24] In the general press, the term GRID, which stood for Gay-related immune deficiency, had been coined.[25] However, after determining that AIDS was not isolated to the homosexual community,[24] the term GRID became misleading and AIDS was introduced at a meeting in July 1982.[26] By September 1982 the CDC started using the name AIDS, and properly defined the illness.[27] In 1993, the CDC expanded their definition of AIDS to include all HIV positive people with a CD4+ T cell count below 200 per µL of blood or 14% of all lymphocytes.[28] The majority of new AIDS cases in developed countries use either this definition or the pre-1993 CDC definition. The AIDS diagnosis still stands even if, after treatment, the CD4+ T cell count rises to above 200 per µL of blood or other AIDS-defining illnesses are cured.
HIV test
Main article: HIV test
Many people are unaware that they are infected with HIV.[29] Less than 1% of the sexually active urban population in Africa has been tested, and this proportion is even lower in rural populations. Furthermore, only 0.5% of pregnant women attending urban health facilities are counseled, tested or receive their test results. Again, this proportion is even lower in rural health facilities.[29] Therefore, donor blood and blood products used in medicine and medical research are screened for HIV. Typical HIV tests, including the HIV enzyme immunoassay and the Western blot assay, detect HIV antibodies in serum, plasma, oral fluid, dried blood spot or urine of patients. However, the window period (the time between initial infection and the development of detectable antibodies against the infection) can vary. This is why it can take 3–6 months to seroconvert and test positive. Commercially available tests to detect other HIV antigens, HIV-RNA, and HIV-DNA in order to detect HIV infection prior to the development of detectable antibodies are available. For the diagnosis of HIV infection these assays are not specifically approved, but are nonetheless routinely used in developed countries.
Transmission and prevention
The three main transmission routes of HIV are sexual contact, exposure to infected body fluids or tissues, and from mother to fetus or child during perinatal period. It is possible to find HIV in the saliva, tears, and urine of infected individuals, but there are no recorded cases of infection by these secretions, and the risk of infection is negligible.[59]
Sexual contact
The majority of HIV infections are acquired through unprotected sexual relations between partners, one of whom has HIV. The primary mode of HIV infection worldwide is through sexual contact between members of the opposite sex.[60][61][62] Sexual transmission occurs with the contact between sexual secretions of one partner with the rectal, genital or oral mucous membranes of another. Unprotected receptive sexual acts are riskier than unprotected insertive sexual acts, with the risk for transmitting HIV from an infected partner to an uninfected partner through unprotected anal intercourse greater than the risk for transmission through vaginal intercourse or oral sex. Oral sex is not without its risks as HIV is transmissible through both insertive and receptive oral sex.[63] The risk of HIV transmission from exposure to saliva is considerably smaller than the risk from exposure to semen; contrary to popular belief, one would have to swallow gallons of saliva from a carrier to run a significant risk of becoming infected.[64]
Approximately 30% of women in ten countries representing "diverse cultural, geographical and urban/rural settings" report that their first sexual experience was forced or coerced, making sexual violence a key driver of the HIV/AIDS pandemic.[65] Sexual assault greatly increases the risk of HIV transmission as protection is rarely employed and physical trauma to the vaginal cavity frequently occurs which facilitates the transmission of HIV.[66]
Sexually transmitted infections (STI) increase the risk of HIV transmission and infection because they cause the disruption of the normal epithelial barrier by genital ulceration and/or microulceration; and by accumulation of pools of HIV-susceptible or HIV-infected cells (lymphocytes and macrophages) in semen and vaginal secretions. Epidemiological studies from sub-Saharan Africa, Europe and North America have suggested that there is approximately a four times greater risk of becoming infected with HIV in the presence of a genital ulcer such as those caused by syphilis and/or chancroid. There is also a significant though lesser increased risk in the presence of STIs such as gonorrhea, Chlamydial infection and trichomoniasis which cause local accumulations of lymphocytes and macrophages.[67]
Transmission of HIV depends on the infectiousness of the index case and the susceptibility of the uninfected partner. Infectivity seems to vary during the course of illness and is not constant between individuals. An undetectable plasma viral load does not necessarily indicate a low viral load in the seminal liquid or genital secretions. Each 10-fold increment of blood plasma HIV RNA is associated with an 81% increased rate of HIV transmission.[67][68] Women are more susceptible to HIV-1 infection due to hormonal changes, vaginal microbial ecology and physiology, and a higher prevalence of sexually transmitted diseases.[69][70] People who are infected with HIV can still be infected by other, more virulent strains.
During a sexual act, only male or female condoms can reduce the chances of infection with HIV and other STDs and the chances of becoming pregnant. The best evidence to date indicates that typical condom use reduces the risk of heterosexual HIV transmission by approximately 80% over the long-term, though the benefit is likely to be higher if condoms are used correctly on every occasion.[71] The effective use of condoms and screening of blood transfusion in North America, Western and Central Europe is credited with contributing to the low rates of AIDS in these regions. Promoting condom use, however, has often proved controversial and difficult. Many religious groups, most noticeably the Roman Catholic Church, have opposed the use of condoms on religious grounds, and have sometimes seen condom promotion as an affront to the promotion of marriage, monogamy and sexual morality. Defenders of the Catholic Church's role in AIDS and general STD prevention state that, while they may be against the use of contraception, they are strong advocates of abstinence outside marriage.[72] This attitude is also found among some health care providers and policy makers in sub-Saharan African nations, where HIV and AIDS prevalence is extremely high.[73] They also believe that the distribution and promotion of condoms is tantamount to promoting sex amongst the youth and sending the wrong message to uninfected individuals. However, no evidence has been produced that promotion of condom use increases sexual promiscuity,[74] and abstinence-only programs have been unsuccessful in the United States both in changing sexual behavior and in reducing HIV transmission.[75] Evaluations of several abstinence-only programs in the US showed a negative impact on the willingness of youths to use contraceptives, due to the emphasis on contraceptives' failure rates.[76] The male latex condom, if used correctly without oil-based lubricants, is the single most effective available technology to reduce the sexual transmission of HIV and other sexually transmitted infections. Manufacturers recommend that oil-based lubricants such as petroleum jelly, butter, and lard not be used with latex condoms, because they dissolve the latex, making the condoms porous. If necessary, manufacturers recommend using water-based lubricants. Oil-based lubricants can however be used with polyurethane condoms.[77] Latex condoms degrade over time, making them porous, which is why condoms have expiration dates. In Europe and the United States, condoms have to conform to European (EC 600) or American (D3492) standards to be considered protective against HIV transmission.
The female condom is an alternative to the male condom and is made from polyurethane, which allows it to be used in the presence of oil-based lubricants. They are larger than male condoms and have a stiffened ring-shaped opening, and are designed to be inserted into the vagina. The female condom contains an inner ring, which keeps the condom in place inside the vagina — inserting the female condom requires squeezing this ring. However, at present availability of female condoms is very low and the price remains prohibitive for many women. Preliminary studies suggest that, where female condoms are available, overall protected sexual acts increase relative to unprotected sexual acts, making them an important HIV prevention strategy.[78]
With consistent and correct use of condoms, there is a very low risk of HIV infection. Studies on couples where one partner is infected show that with consistent condom use, HIV infection rates for the uninfected partner are below 1% per year.[79]
The United States government and health organizations both endorse the ABC Approach to lower the risk of acquiring AIDS during sex:
Abstinence or delay of sexual activity, especially for youth,
Being faithful, especially for those in committed relationships,
Condom use, for those who engage in risky behavior.
This approach has been very successful in Uganda, where HIV prevalence has decreased from 15% to 5%. However, more has been done than just this. As Edward Green, a Harvard medical anthropologist, put it, "Uganda has pioneered approaches towards reducing stigma, bringing discussion of sexual behavior out into the open, involving HIV-infected people in public education, persuading individuals and couples to be tested and counseled, improving the status of women, involving religious organizations, enlisting traditional healers, and much more." However, criticism of the ABC approach is widespread because a faithful partner of an unfaithful partner is at risk of contracting HIV and that discrimination against women and girls is so great that they are without voice in almost every area of their lives.[80] Other programs and initiatives promote condom use more heavily. Condom use is an integral part of the CNN Approach. This is:
Condom use, for those who engage in risky behavior,
Needles, use clean ones,
Negotiating skills; negotiating safer sex with a partner and empowering women to make smart choices.
In December 2006, the last of three large, randomized trials confirmed that male circumcision lowers the risk of HIV infection among heterosexual African men by around 50%. It is expected that this intervention will be actively promoted in many of the countries worst affected by HIV, although doing so will involve confronting a number of practical, cultural and attitudinal issues. Some experts fear that a lower perception of vulnerability among circumcised men may result in more sexual risk-taking behavior, thus negating its preventive effects.[81] Furthermore, South African medical experts are concerned that the repeated use of unsterilized blades in the ritual circumcision of adolescent boys may be spreading HIV.
This transmission route is particularly relevant to intravenous drug users, hemophiliacs and recipients of blood transfusions and blood products. Sharing and reusing syringes contaminated with HIV-infected blood represents a major risk for infection with not only HIV, but also hepatitis B and hepatitis C. Needle sharing is the cause of one third of all new HIV-infections and 50% of hepatitis C infections in North America, China, and Eastern Europe. The risk of being infected with HIV from a single prick with a needle that has been used on an HIV-infected person is thought to be about 1 in 150 (see table above). Post-exposure prophylaxis with anti-HIV drugs can further reduce that small risk.[83] Health care workers (nurses, laboratory workers, doctors etc) are also concerned, although more rarely. This route can affect people who give and receive tattoos and piercings. Universal precautions are frequently not followed in both sub-Saharan Africa and much of Asia because of both a shortage of supplies and inadequate training. The WHO estimates that approximately 2.5% of all HIV infections in sub-Saharan Africa are transmitted through unsafe healthcare injections.[84] Because of this, the United Nations General Assembly, supported by universal medical opinion on the matter, has urged the nations of the world to implement universal precautions to prevent HIV transmission in health care settings.[85] Drug abuse has an additional effect of an increased tendency to engage in unprotected sexual intercourse [86].
The risk of transmitting HIV to blood transfusion recipients is extremely low in developed countries where improved donor selection and HIV screening is performed. However, according to the WHO, the overwhelming majority of the world's population does not have access to safe blood and "between 5% and 10% of HIV infections worldwide are transmitted through the transfusion of infected blood and blood products".[87]
Medical workers who follow universal precautions or body-substance isolation, such as wearing latex gloves when giving injections and washing the hands frequently, can help prevent infection by HIV.
All AIDS-prevention organizations advise drug-users not to share needles and other material required to prepare and take drugs (including syringes, cotton balls, the spoons, water for diluting the drug, straws, crack pipes, etc). It is important that people use new or properly sterilized needles for each injection. Information on cleaning needles using bleach is available from health care and addiction professionals and from needle exchanges. In some developed countries, clean needles are available free in some cities, at needle exchanges or safe injection sites. Additionally, many nations have decriminalized needle possession and made it possible to buy injection equipment from pharmacists without a prescription.
Mother-to-child transmission (MTCT)
The transmission of the virus from the mother to the child can occur in utero during the last weeks of pregnancy and at childbirth. In the absence of treatment, the transmission rate between the mother to the child during pregnancy, labor and delivery is 25%. However, when the mother has access to antiretroviral therapy and gives birth by caesarean section, the rate of transmission is just 1%.[53] A number of factors influence the risk of infection, particularly the viral load of the mother at birth (the higher the viral load, the higher the risk). Breastfeeding increases the risk of transmission by 10–15%. This risk depends on clinical factors and may vary according to the pattern and duration of breast-feeding.
Studies have shown that antiretroviral drugs, caesarean delivery and formula feeding reduce the chance of transmission of HIV from mother to child.[88] Current recommendations state that when replacement feeding is acceptable, feasible, affordable, sustainable and safe, HIV-infected mothers should avoid breast-feeding their infant. However, if this is not the case, exclusive breast-feeding is recommended during the first months of life and discontinued as soon as possible.[6] In 2005, around 700,000 children under 15 contracted HIV, mainly through MTCT, with 630,000 of these infections occurring in Africa.[89] Of the children currently living with HIV, 2 million (almost 90%) live in sub-Saharan Africa.[6]
Prevention strategies are well known in developed countries, however, recent epidemiological and behavioral studies in Europe and North America have suggested that a substantial minority of young people continue to engage in high-risk practices and that despite HIV/AIDS knowledge, young people underestimate their own risk of becoming infected with HIV.[90] However, transmission of HIV between intravenous drug users has clearly decreased, and HIV transmission by blood transfusion has become quite rare in developed countries.
Treatment
There is currently no vaccine or cure for HIV or AIDS. The only known methods of prevention are based on avoiding exposure to the virus or, failing that, an antiretroviral treatment directly after a highly significant exposure, called post-exposure prophylaxis (PEP).[83] PEP has a very demanding four week schedule of dosage. It also has very unpleasant side effects including diarrhea, malaise, nausea and fatigue.[91]
Current treatment for HIV infection consists of highly active antiretroviral therapy, or HAART.[92] This has been highly beneficial to many HIV-infected individuals since its introduction in 1996 when the protease inhibitor-based HAART initially became available.[7] Current optimal HAART options consist of combinations (or "cocktails") consisting of at least three drugs belonging to at least two types, or "classes," of antiretroviral agents. Typical regimens consist of two nucleoside analogue reverse transcriptase inhibitors (NARTIs or NRTIs) plus either a protease inhibitor or a non-nucleoside reverse transcriptase inhibitor (NNRTI). Because HIV disease progression in children is more rapid than in adults, and laboratory parameters are less predictive of risk for disease progression, particularly for young infants, treatment recommendations are more aggressive for children than for adults.[93] In developed countries where HAART is available, doctors assess the viral load, rapidity in CD4 decline, and patient readiness while deciding when to recommend initiating treatment.[94]
HAART allows the stabilization of the patient’s symptoms and viremia, but it neither cures the patient of HIV, nor alleviates the symptoms, and high levels of HIV-1, often HAART resistant, return once treatment is stopped.[95][96] Moreover, it would take more than the lifetime of an individual to be cleared of HIV infection using HAART.[97] Despite this, many HIV-infected individuals have experienced remarkable improvements in their general health and quality of life, which has led to the plummeting of HIV-associated morbidity and mortality.[98][99][100] In the absence of HAART, progression from HIV infection to AIDS occurs at a median of between nine to ten years and the median survival time after developing AIDS is only 9.2 months.[12] HAART is thought to increase survival time by between 4 and 12 years.[101][102] This average reflects the fact that for some patients — and in many clinical cohorts this may be more than fifty percent of patients — HAART achieves far less than optimal results. This is due to a variety of reasons such as medication intolerance/side effects, prior ineffective antiretroviral therapy and infection with a drug-resistant strain of HIV. However, non-adherence and non-persistence with antiretroviral therapy is the major reason most individuals fail to get any benefit from and develop resistance to HAART.[103] The reasons for non-adherence and non-persistence with HAART are varied and overlapping. Major psychosocial issues, such as poor access to medical care, inadequate social supports, psychiatric disease and drug abuse contribute to non-adherence. The complexity of these HAART regimens, whether due to pill number, dosing frequency, meal restrictions or other issues, along with side effects that create intentional non-adherence, also has a weighty impact.[104][105][106] The side effects include lipodystrophy, dyslipidaemia, insulin resistance, an increase in cardiovascular risks and birth defects.[107][108]
Daily multivitamin and mineral supplements have been found to reduce HIV disease progression among men and women. This could become an important low-cost intervention provided during early HIV disease to prolong the time before antiretroviral therapy is required.[109] Some individual nutrients have also been tried.[110][111] Anti-retroviral drugs are expensive, and the majority of the world's infected individuals do not have access to medications and treatments for HIV and AIDS.[112] It has been postulated that only a vaccine can halt the pandemic because a vaccine would possibly cost less, thus being affordable for developing countries, and would not require daily treatments.[112] However, after over 20 years of research, HIV-1 remains a difficult target for a vaccine.[112]
Research to improve current treatments includes decreasing side effects of current drugs, further simplifying drug regimens to improve adherence, and determining the best sequence of regimens to manage drug resistance. A number of studies have shown that measures to prevent opportunistic infections can be beneficial when treating patients with HIV infection or AIDS. Vaccination against hepatitis A and B is advised for patients who are not infected with these viruses and are at risk of becoming infected.[113] Patients with substantial immunosuppression are also advised to receive prophylactic therapy for Pneumocystis jiroveci pneumonia (PCP), and many patients may benefit from prophylactic therapy for toxoplasmosis and Cryptococcus meningitis as well.[91]
Various forms of alternative medicine have been tried to treat symptoms or alter the course of the disease.[114] In the first decade of the epidemic when no useful conventional treatment was available, a large number of people with AIDS experimented with alternative therapies. The definition of "alternative therapies" in AIDS has changed since that time. Then, the phrase often referred to community-driven treatments, untested by government or pharmaceutical company research, that some hoped would directly suppress the virus or stimulate immunity against it. Examples of alternative medicine that people hoped would improve their symptoms or their quality of life include massage, stress management, herbal and flower remedies such as boxwood,[115][116] and acupuncture;[114] when used with conventional treatment, many now refer to these as "complementary" approaches. Despite the widespread use of complementary and alternative medicine by people living with HIV/AIDS, the effectiveness of these therapies has not been established.
Dengue fever
Dengue fever (IPA: /ˈdɛŋgeɪ/) and dengue hemorrhagic fever (DHF) are acute febrile diseases, found in the tropics and Africa, with a geographical spread similar to malaria.[1] One major difference, however, is that malaria is often eradicated in major cities, whereas dengue is often found in urban areas of developed tropical nations, including Singapore, Taiwan, Indonesia, and Brazil. Caused by one of four closely related virus serotypes of the genus Flavivirus, family Flaviviridae, each serotype is sufficiently different that there is no cross-protection and epidemics caused by multiple serotypes (hyperendemicity) can occur. Dengue is transmitted to humans by the Aedes aegypti (rarely Aedes albopictus) mosquito, which feeds during the day.
Signs and symptoms
This infectious disease is manifested by a sudden onset of fever, with severe headache, muscle and joint pains (myalgias and arthralgias—severe pain gives it the name break-bone fever or bonecrusher disease) and rashes. The dengue rash is characteristically bright red petechia and usually appears first on the lower limbs and the chest; in some patients, it spreads to cover most of the body. There may also be gastritis with some combination of associated abdominal pain, nausea, vomiting or diarrhea.
Some cases develop much milder symptoms which can, when no rash is present, be misdiagnosed as influenza or other viral infection. Thus travelers from tropical areas may inadvertently pass on dengue in their home countries, having not been properly diagnosed at the height of their illness. Patients with dengue can pass on the infection only through mosquitoes or blood products and only while they are still febrile.
The classic dengue fever lasts about six to seven days, with a smaller peak of fever at the trailing end of the disease (the so-called "biphasic pattern"). Clinically, the platelet count will drop until the patient's temperature is normal.
Cases of DHF also show higher fever, haemorrhagic phenomena, thrombocytopenia, and haemoconcentration. A small proportion of cases lead to dengue shock syndrome (DSS) which has a high mortality rate.
Diagnosis
The diagnosis of dengue is usually made clinically. The classic picture is high fever with no localising source of infection, a petechial rash with thrombocytopenia and relative leukopenia.
The WHO definition of dengue haemorrhagic fever has been in use since 1975; all four criteria must be fulfilled:
1. Fever
2. Hemorrhagic tendency (positive tourniquet test, spontaneous bruising, bleeding from mucosa, gingiva, injection sites, etc.; vomiting blood, or bloody diarrhea)
3. Thrombocytopenia (<100,000 platelets per mm³ or estimated as less than 3 platelets per high power field)
4. Evidence of plasma leakage (hematocrit more than 20% higher than expected, or drop in haematocrit of 20% or more from baseline following IV fluid, pleural effusion, ascites, hypoproteinemia)
Dengue shock syndrome is defined as dengue hemorrhagic fever plus:
* Weak rapid pulse,
* Narrow pulse pressure (less than 20 mm Hg) or,
* Cold, clammy skin and restlessness.
Serology and PCR (polymerase chain reaction) studies are available to confirm the diagnosis of dengue if clinically indicated.
Treatment
The mainstay of treatment is supportive therapy. Increased oral fluid intake is recommended to prevent dehydration. Supplementation with intravenous fluids may be necessary to prevent dehydration and significant concentration of the blood if the patient is unable to maintain oral intake. A platelet transfusion is indicated in rare cases if the platelet level drops significantly (below 20,000) or if there is significant bleeding.
The presence of melena may indicate internal gastrointestinal bleeding requiring platelet and/or red blood cell transfusion.
It is very important to avoid aspirin and non-steroidal anti-inflammatory drugs; these drugs may aggravate the bleeding tendency associated with some of these infections. Patients should receive instead acetaminophen preparations to deal with these symptoms if dengue is suspected.
Emerging treatments
Emerging evidence suggests that mycophenolic acid and ribavirin inhibit dengue replication. Initial experiments showed a fivefold increase in defective viral RNA production by cells treated with each drug.In vivo studies, however, have not yet been done.
Friday, February 22, 2008
Pneumonia

Pneumonia is an inflammatory illness of the lung.[1] Frequently, it is described as lung parenchyma/alveolar (microscopic air-filled sacs of the lung responsible for absorbing oxygen from the atmosphere) inflammation and (abnormal) alveolar filling with fluid. Pneumonia can result from a variety of causes, including infection with bacteria, viruses, fungi, or parasites, and chemical or physical injury to the lungs. Its cause may also be officially described as idiopathic--that is, unknown--when infectious causes have been excluded.
Typical symptoms associated with pneumonia include cough, chest pain, fever, and difficulty in breathing. Diagnostic tools include x-rays and examination of the sputum. Treatment depends on the cause of pneumonia; bacterial pneumonia is treated with antibiotics.
Pneumonia is a common illness which occurs in all age groups, and is a leading cause of death among the elderly and people who are chronically and terminally ill. Vaccines to prevent certain types of pneumonia are available. The prognosis depends on the type of pneumonia, the appropriate treatment, any complications, and the person's underlying health.
Malaria

Malaria is a vector-borne infectious disease caused by protozoan parasites. It is widespread in tropical and subtropical regions, including parts of the Americas, Asia, and Africa. Each year, it causes disease in approximately 515 million people and kills between one and three million people, the majority of whom are young children in Sub-Saharan Africa.[1] Malaria is commonly associated with poverty, but is also a cause of poverty and a major hindrance to economic development.
Malaria is one of the most common infectious diseases and an enormous public health problem. The disease is caused by protozoan parasites of the genus Plasmodium. Only four types of the plasmodium parasite can infect humans; the most serious forms of the disease are caused by Plasmodium falciparum and Plasmodium vivax, but other related species (Plasmodium ovale, Plasmodium malariae) can also affect humans. This group of human-pathogenic Plasmodium species is usually referred to as malaria parasites.
Malaria parasites are transmitted by female Anopheles mosquitoes. The parasites multiply within red blood cells, causing symptoms that include symptoms of anemia (light headedness, shortness of breath, tachycardia etc.), as well as other general symptoms such as fever, chills, nausea, flu-like illness, and in severe cases, coma and death. Malaria transmission can be reduced by preventing mosquito bites with mosquito nets and insect repellents, or by mosquito control measures such as spraying insecticides inside houses and draining standing water where mosquitoes lay their eggs.
Although some are under development, no vaccine is currently available for malaria; preventative drugs must be taken continuously to reduce the risk of infection. These prophylactic drug treatments are often too expensive for most people living in endemic areas. Most adults from endemic areas have a degree of long-term recurrent infection and also of partial resistance; the resistance reduces with time and such adults may become susceptible to severe malaria if they have spent a significant amount of time in non-endemic areas. They are strongly recommended to take full precautions if they return to an endemic area. Malaria infections are treated through the use of antimalarial drugs, such as quinine or artemisinin derivatives, although drug resistance is increasingly common.
Symptoms
Symptoms of malaria include fever, shivering, arthralgia (joint pain), vomiting, anemia (caused by hemolysis), hemoglobinuria, and convulsions. There may be the feeling of tingling in the skin, particularly with malaria caused by P. falciparum. The classical symptom of malaria is cyclical occurrence of sudden coldness followed by rigor and then fever and sweating lasting four to six hours, occurring every two days in P. vivax and P. ovale infections, while every three for P. malariae.[30] P. falciparum can have recurrent fever every 36-48 hours or a less pronounced and almost continuous fever. For reasons that are poorly understood, but which may be related to high intracranial pressure, children with malaria frequently exhibit abnormal posturing, a sign indicating severe brain damage.[31] Malaria has been found to cause cognitive impairments, especially in children. It causes widespread anemia during a period of rapid brain development and also direct brain damage. This neurologic damage results from cerebral malaria to which children are more vulnerable.[32]
Severe malaria is almost exclusively caused by P. falciparum infection and usually arises 6-14 days after infection.[33] Consequences of severe malaria include coma and death if untreated—young children and pregnant women are especially vulnerable. Splenomegaly (enlarged spleen), severe headache, cerebral ischemia, hepatomegaly (enlarged liver), hypoglycemia, and hemoglobinuria with renal failure may occur. Renal failure may cause blackwater fever, where hemoglobin from lysed red blood cells leaks into the urine. Severe malaria can progress extremely rapidly and cause death within hours or days.[33] In the most severe cases of the disease fatality rates can exceed 20%, even with intensive care and treatment.[34] In endemic areas, treatment is often less satisfactory and the overall fatality rate for all cases of malaria can be as high as one in ten.[35] Over the longer term, developmental impairments have been documented in children who have suffered episodes of severe malaria.[36]
Chronic malaria is seen in both P. vivax and P. ovale, but not in P. falciparum. Here, the disease can relapse months or years after exposure, due to the presence of latent parasites in the liver. Describing a case of malaria as cured by observing the disappearance of parasites from the bloodstream can therefore be deceptive. The longest incubation period reported for a P. vivax infection is 30 years.[33] Approximately one in five of P. vivax malaria cases in temperate areas involve overwintering by hypnozoites (i.e., relapses begin the year after the mosquito bite).
Causes
Malaria parasites
Malaria is caused by protozoan parasites of the genus Plasmodium (phylum Apicomplexa). In humans malaria is caused by P. falciparum, P. malariae, P. ovale, and P. vivax. P. falciparum is the most common cause of infection, responsible for about 80 % of all malaria cases. However, P. falciparum is the most important cause of disease, and responsible for about 90% of deaths.[38] Parasitic Plasmodium species also infect birds, reptiles, monkeys, chimpanzees and rodents.[39] There have been documented human infections with several simian species of malaria, namely P. knowlesi, P. inui, P. cynomolgi,[40] P. simiovale, P. brazilianum, P. schwetzi and P. simium; however these are mostly of limited public health importance. Although avian malaria can kill chickens and turkeys, this disease does not cause serious economic losses to poultry farmers.[41] However, since being accidentally introduced by humans it has decimated the endemic birds of Hawaii, which evolved in its absence and lack any resistance to it.
Diagnosis
The most economic, preferred, and reliable diagnosis of malaria is microscopic examination of blood films because each of the four major parasite species has distinguishing characteristics. Two sorts of blood film are traditionally used. Thin films are similar to usual blood films and allow species identification because the parasite's appearance is best preserved in this preparation. Thick films allow the microscopist to screen a larger volume of blood and are about eleven times more sensitive than the thin film, so picking up low levels of infection is easier on the thick film, but the appearance of the parasite is much more distorted and therefore distinguishing between the different species can be much more difficult. With the pros and cons of both thick and thin smears taken into consideration, it is imperative to utilize both smears while attempting to make a definitive diagnosis.
From the thick film, an experienced microscopist can detect parasite levels (or parasitemia) down to as low as 0.0000001% of red blood cells. Microscopic diagnosis can be difficult because the early trophozoites ("ring form") of all four species look identical and it is never possible to diagnose species on the basis of a single ring form; species identification is always based on several trophozoites. Please refer to the articles on each parasite for their microscopic appearances: P. falciparum, P. vivax, P. ovale, P. malariae.
In areas where microscopy is not available, or where laboratory staff are not experienced at malaria diagnosis, there are antigen detection tests that require only a drop of blood.[57] OptiMAL-IT® will reliably detect falciparum down to 0.01% parasitemia and non-falciparum down to 0.1%. Paracheck-Pf® will detect parasitemias down to 0.002% but will not distinguish between falciparum and non-falciparum malaria. Parasite nucleic acids are detected using polymerase chain reaction. This technique is more accurate than microscopy. However, it is expensive, and requires a specialized laboratory. Moreover, levels of parasitemia are not necessarily correlative with the progression of disease, particularly when the parasite is able to adhere to blood vessel walls. Therefore more sensitive, low-tech diagnosis tools need to be developed in order to detect low levels of parasitaemia in the field. Areas that cannot afford even simple laboratory diagnostic tests often use only a history of subjective fever as the indication to treat for malaria. Using Giemsa-stained blood smears from children in Malawi, one study showed that unnecessary treatment for malaria was significantly decreased when clinical predictors (rectal temperature, nailbed pallor, and splenomegaly) were used as treatment indications, rather than the current national policy of using only a history of subjective fevers (sensitivity increased from 21% to 41%).
Molecular methods are available in some clinical laboratories and rapid real-time assays (for example, QT-NASBA based on the polymerase chain reaction)are being developed with the hope of being able to deploy them in endemic areas.
Severe malaria is commonly misdiagnosed in Africa, leading to a failure to treat other life-threatening illnesses. In malaria-endemic areas, parasitemia does not ensure a diagnosis of severe malaria because parasitemia can be incidental to other concurrent disease. Recent investigations suggest that malarial retinopathy is better (collective sensitivity of 95% and specificity of 90%) than any other clinical or laboratory feature in distinguishing malarial from non-malarial coma.
Treatment
Active malaria infection with P. falciparum is a medical emergency requiring hospitalization. Infection with P. vivax, P. ovale or P. malariae can often be treated on an outpatient basis. Treatment of malaria involves supportive measures as well as specific antimalarial drugs. When properly treated, someone with malaria can expect a complete cure.
Antimalarial drugs
Further information: Antimalarial drugs
There are several families of drugs used to treat malaria. Chloroquine is very cheap and, until recently, was very effective, which made it the antimalarial drug of choice for many years in most parts of the world. However, resistance of Plasmodium falciparum to chloroquine has spread recently from Asia to Africa, making the drug ineffective against the most dangerous Plasmodium strain in many affected regions of the world. In those areas where chloroquine is still effective it remains the first choice. Unfortunately, chloroquine-resistance is associated with reduced sensitivity to other drugs such as quinine and amodiaquine.
There are several other substances which are used for treatment and, partially, for prevention (prophylaxis). Many drugs may be used for both purposes; larger doses are used to treat cases of malaria. Their deployment depends mainly on the frequency of resistant parasites in the area where the drug is used. One drug currently being investigated for possible use as an anti-malarial, especially for treatment of drug-resistant strains, is the beta blocker propranolol. Propranolol has been shown to block both Plasmodium's ability to enter red blood cell and establish an infection, as well as parasite replication. A December 2006 study by Northwestern University researchers suggested that propranolol may reduce the dosages required for existing drugs to be effective against P. falciparum by 5- to 10-fold, suggesting a role in combination therapies.
Currently available anti-malarial drugs include:
* Artemether-lumefantrine (Therapy only, commercial names Coartem® and Riamet®)
* Artesunate-amodiaquine (Therapy only)
* Artesunate-mefloquine (Therapy only)
* Artesunate-Sulfadoxine/pyrimethamine (Therapy only)
* Atovaquone-proguanil, trade name Malarone (Therapy and prophylaxis)
* Quinine (Therapy only)
* Chloroquine (Therapy and prophylaxis; usefulness now reduced due to resistance)
* Cotrifazid (Therapy and prophylaxis)
* Doxycycline (Therapy and prophylaxis)
* Mefloquine, trade name Lariam (Therapy and prophylaxis)
* Primaquine (Therapy in P. vivax and P. ovale only; not for prophylaxis)
* Proguanil (Prophylaxis only)
* Sulfadoxine-pyrimethamine (Therapy; prophylaxis for semi-immune pregnant women in endemic countries as "Intermittent Preventive Treatment" - IPT)
* Hydroxychloroquine, trade name Plaquenil (Therapy and prophylaxis)
The development of drugs was facilitated when Plasmodium falciparum was successfully cultured.[65] This allowed in vitro testing of new drug candidates.
Extracts of the plant Artemisia annua, containing the compound artemisinin or semi-synthetic derivatives (a substance unrelated to quinine), offer over 90% efficacy rates, but their supply is not meeting demand.[66] One study in Rwanda showed that children with uncomplicated P. falciparum malaria demonstrated fewer clinical and parasitological failures on post-treatment day 28 when amodiaquine was combined with artesunate, rather than administered alone (OR = 0.34). However, increased resistance to amodiaquine during this study period was also noted.[67] Since 2001 the World Health Organization has recommended using artemisinin-based combination therapy (ACT) as first-line treatment for uncomplicated malaria in areas experiencing resistance to older medications. The most recent WHO treatment guidelines for malaria recommend four different ACTs. While numerous countries, including most African nations, have adopted the change in their official malaria treatment policies, cost remains a major barrier to ACT implementation. Because ACTs cost up to twenty times as much as older medications, they remain unaffordable in many malaria-endemic countries. The molecular target of artemisinin is controversial, although recent studies suggest that SERCA, a calcium pump in the endoplasmic reticulum may be associated with artemisinin resistance.[68] Malaria parasites can develop resistance to artemisinin and resistance can be produced by mutation of SERCA.[69] However, other studies suggest the mitochondrion is the major target for artemisinin and its analogs.
In February 2002, the journal Science and other press outlets[71] announced progress on a new treatment for infected individuals. A team of French and South African researchers had identified a new drug they were calling "G25".[72] It cured malaria in test primates by blocking the ability of the parasite to copy itself within the red blood cells of its victims. In 2005 the same team of researchers published their research on achieving an oral form, which they refer to as "TE3" or "te3".[73] As of early 2006, there is no information in the mainstream press as to when this family of drugs will become commercially available.
In 1996, Professor Geoff McFadden stumbled upon the work of British biologist Ian Wilson, who had discovered that the plasmodia responsible for causing malaria retained parts of chloroplasts,[74] an organelle usually found in plants, complete with their own functioning genomes. This led Professor McFadden to the realisation that any number of herbicides may in fact be successful in the fight against malaria, and so he set about trialing large numbers of them, and enjoyed a 75% success rate.
These "apicoplasts" are thought to have originated through the endosymbiosis of algae[75] and play a crucial role in fatty acid bio-synthesis in plasmodia.[76] To date, 466 proteins have been found to be produced by apicoplasts[77] and these are now being looked at as possible targets for novel anti-malarial drugs.
Although effective anti-malarial drugs are on the market, the disease remains a threat to people living in endemic areas who have no proper and prompt access to effective drugs. Access to pharmacies and health facilities, as well as drug costs, are major obstacles. Médecins Sans Frontières estimates that the cost of treating a malaria-infected person in an endemic country was between US$0.25 and $2.40 per dose in 2002.
Counterfeit drugs
Sophisticated counterfeits have been found in Thailand, Vietnam, Cambodia[79] and China,[80] and are an important cause of avoidable death in these countries.[81] There is no reliable way for doctors or lay people to detect counterfeit drugs without help from a laboratory. Companies are attempting to combat the persistence of counterfeit drugs by using new technology to provide security from source to distribution.
Prevention and disease control
Methods used to prevent the spread of disease, or to protect individuals in areas where malaria is endemic, include prophylactic drugs, mosquito eradication, and the prevention of mosquito bites. There is currently no vaccine that will prevent malaria, but this is an active field of research.
Many researchers argue that prevention of malaria may be more cost-effective than treatment of the disease in the long run, but the capital costs required are out of reach of many of the world's poorest people. Economic adviser Jeffrey Sachs estimates that malaria can be controlled for US$3 billion in aid per year. It has been argued that, in order to meet the Millennium Development Goals, money should be redirected from HIV/AIDS treatment to malaria prevention, which for the same amount of money would provide greater benefit to African economies.[82]
Efforts to eradicate malaria by eliminating mosquitoes have been successful in some areas. Malaria was once common in the United States and southern Europe, but the draining of wetland breeding grounds and better sanitation, in conjunction with the monitoring and treatment of infected humans, eliminated it from affluent regions. In 2002, there were 1,059 cases of malaria reported in the US, including eight deaths. In five of those cases, the disease was contracted in the United States. Malaria was eliminated from the northern parts of the USA in the early twentieth century, and the use of the pesticide DDT eliminated it from the South by 1951. In the 1950s and 1960s, there was a major public health effort to eradicate malaria worldwide by selectively targeting mosquitoes in areas where malaria was rampant.[83] However, these efforts have so far failed to eradicate malaria in many parts of the developing world - the problem is most prevalent in Africa.
Brazil, Eritrea, India, and Vietnam have, unlike many other developing nations, successfully reduced the malaria burden. Common success factors included conducive country conditions, a targeted technical approach using a package of effective tools, data-driven decision-making, active leadership at all levels of government, involvement of communities, decentralized implementation and control of finances, skilled technical and managerial capacity at national and sub-national levels, hands-on technical and programmatic support from partner agencies, and sufficient and flexible financing.[84]
The Malaria Control Project is currently using downtime computing power donated by individual volunteers around the world (see Volunteer computing and BOINC) to simulate models of the health effects and transmission dynamics in order to find the best method or combination of methods for malaria control. This modeling is extremely computer intensive due to the simulations of large human populations with a vast range of parameters related to biological and social factors that influence the spread of the disease. It is expected to take a few months using volunteered computing power compared to the 40 years it would have taken with the current resources available to the scientists who developed the program.
Subscribe to:
Posts (Atom)