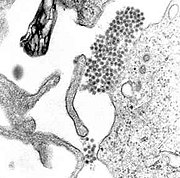
Dengue fever (IPA: /ˈdɛŋgeɪ/) and dengue hemorrhagic fever (DHF) are acute febrile diseases, found in the tropics and Africa, with a geographical spread similar to malaria.[1] One major difference, however, is that malaria is often eradicated in major cities, whereas dengue is often found in urban areas of developed tropical nations, including Singapore, Taiwan, Indonesia, and Brazil. Caused by one of four closely related virus serotypes of the genus Flavivirus, family Flaviviridae, each serotype is sufficiently different that there is no cross-protection and epidemics caused by multiple serotypes (hyperendemicity) can occur. Dengue is transmitted to humans by the Aedes aegypti (rarely Aedes albopictus) mosquito, which feeds during the day.
Signs and symptoms
This infectious disease is manifested by a sudden onset of fever, with severe headache, muscle and joint pains (myalgias and arthralgias—severe pain gives it the name break-bone fever or bonecrusher disease) and rashes. The dengue rash is characteristically bright red petechia and usually appears first on the lower limbs and the chest; in some patients, it spreads to cover most of the body. There may also be gastritis with some combination of associated abdominal pain, nausea, vomiting or diarrhea.
Some cases develop much milder symptoms which can, when no rash is present, be misdiagnosed as influenza or other viral infection. Thus travelers from tropical areas may inadvertently pass on dengue in their home countries, having not been properly diagnosed at the height of their illness. Patients with dengue can pass on the infection only through mosquitoes or blood products and only while they are still febrile.
The classic dengue fever lasts about six to seven days, with a smaller peak of fever at the trailing end of the disease (the so-called "biphasic pattern"). Clinically, the platelet count will drop until the patient's temperature is normal.
Cases of DHF also show higher fever, haemorrhagic phenomena, thrombocytopenia, and haemoconcentration. A small proportion of cases lead to dengue shock syndrome (DSS) which has a high mortality rate.
Diagnosis
The diagnosis of dengue is usually made clinically. The classic picture is high fever with no localising source of infection, a petechial rash with thrombocytopenia and relative leukopenia.
The WHO definition of dengue haemorrhagic fever has been in use since 1975; all four criteria must be fulfilled:
1. Fever
2. Hemorrhagic tendency (positive tourniquet test, spontaneous bruising, bleeding from mucosa, gingiva, injection sites, etc.; vomiting blood, or bloody diarrhea)
3. Thrombocytopenia (<100,000 platelets per mm³ or estimated as less than 3 platelets per high power field)
4. Evidence of plasma leakage (hematocrit more than 20% higher than expected, or drop in haematocrit of 20% or more from baseline following IV fluid, pleural effusion, ascites, hypoproteinemia)
Dengue shock syndrome is defined as dengue hemorrhagic fever plus:
* Weak rapid pulse,
* Narrow pulse pressure (less than 20 mm Hg) or,
* Cold, clammy skin and restlessness.
Serology and PCR (polymerase chain reaction) studies are available to confirm the diagnosis of dengue if clinically indicated.
Treatment
The mainstay of treatment is supportive therapy. Increased oral fluid intake is recommended to prevent dehydration. Supplementation with intravenous fluids may be necessary to prevent dehydration and significant concentration of the blood if the patient is unable to maintain oral intake. A platelet transfusion is indicated in rare cases if the platelet level drops significantly (below 20,000) or if there is significant bleeding.
The presence of melena may indicate internal gastrointestinal bleeding requiring platelet and/or red blood cell transfusion.
It is very important to avoid aspirin and non-steroidal anti-inflammatory drugs; these drugs may aggravate the bleeding tendency associated with some of these infections. Patients should receive instead acetaminophen preparations to deal with these symptoms if dengue is suspected.
Emerging treatments
Emerging evidence suggests that mycophenolic acid and ribavirin inhibit dengue replication. Initial experiments showed a fivefold increase in defective viral RNA production by cells treated with each drug.In vivo studies, however, have not yet been done.
No comments:
Post a Comment